Abstract
Introduction
Autistic adults experience high rates of co-occurring physical and mental health conditions and often face unmet needs in all healthcare settings due to communication differences, sensory sensitivities, and atypical presentations. Healthcare professionals (HCPs) play a central role in addressing these needs; however, evidence suggests there are significant gaps in autism-specific knowledge and training.
Aim
To examine HCPs' knowledge, experience, and training related to caring for autistic adults.
Methods
A systematic review was conducted according to the PRISMA guidelines. Studies were retrieved from five databases (Scopus, PsycINFO, PubMed, Medline and Web of Science) and nineteen studies were included in the final analysis.
Results
Findings across studies indicated that HCPs possess limited and inconsistent autism-specific knowledge, and have common deficits, with notable gaps in communication, recognition of autistic adults, and management of sensory and co-occurring health needs. Clinical experience caring for autistic adults was variable and often limited. Autism-specific training was inconsistent and typically brief, with between one-third and three-quarters of HCPs reporting unmet training needs.
Conclusion
This review highlighted substantial gaps in HCPs' autism-specific knowledge, experience, and training contributing to barriers in healthcare for autistic adults. Findings highlight a clear need for standardised, competency-based autism education across undergraduate training and continuing professional development. Future research is needed to establish coherent structured curricula with meaningful involvement of autistic adults in the design and delivery of training and education to support person- centred healthcare.
1. Introduction
Autism is a lifelong neurodevelopmental condition with onset in childhood and extends into adulthood (American Psychiatric Association, 2024). However, there is an increasing number of individuals being identified later in life (Fyfe et al., 2026; Lai and Barron-Cohen, 2015). Reported prevalence has risen in recent decades, with the latest reported prevalence of autism in children (aged 8 years) in the US at 32.2 per 1,000 children (Shaw et al., 2025). Among adults, prevalence is estimated at 2.21% in the US, while a UK community-based study reported 9.9 per 1,000 (Brugha et al., 2011). Despite these statistics, healthcare systems often fail to accommodate autistic individuals which contributes to miscommunication and avoidable adverse outcomes (Doherty et al., 2022; Shaw et al., 2024). Autistic adults experience elevated rates of co-occurring physical and mental health conditions, which also contribute to poorer health outcomes. Recognition of these conditions is often challenging due to atypical presentations, communication differences, and sensory processing sensitivities (Bellardinelli et al., 2016). Healthcare professionals (HCPs) play a crucial role in addressing these needs; however, a previous review indicates that autism-specific knowledge can be limited and, in some cases, outdated. Persistent gaps exist in communication strategies, recognition of co-occurring conditions, and the implementation of appropriate care adjustments (Corden et al., 2022). The purpose of this systematic review was to synthesise the existing evidence on HCPs' knowledge, experience and training in caring for autistic adults, with a particular focus on identifying key gaps and informing targeted education and service improvements. This synthesis provides evidence to guide future education and service development aimed at improving care for autistic adults. Recognising that competence in healthcare encompasses knowledge, communication, collaboration, and professionals' behaviours, the Canadian Medical Education Directives for Specialists (CanMEDS) framework provides a widely used model that describes core competencies required of HCPs (Frank et al., 2015). By using this understanding of competence, this review identifies key gaps across HCPs' knowledge, experience and training. Addressing these gaps is essential to improving outcomes, supporting early recognition of health conditions, and enhancing the healthcare experience of autistic adults.
2. Methods
2.1. Research design
A comprehensive systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2020) for reporting of the findings (See Figure 1). The protocol of this systematic review has been registered with PROSPERO (CRD420251120773).
2.2. Search methods
Preliminary searches were conducted using PubMed by F.R. using a list of search terms to identify appropriate terminology related to healthcare access and utilisation among autistic adults. The findings from the preliminary search informed the refinement of the final search terms. A structured search was conducted by F.R. in Scopus, PsycINFO, PubMed, MEDLINE, and Web of Science for studies published from 2013 to 2026. The search strategy combined terms relating to (1) autism, (2) adults, (3) healthcare professionals, and (4) knowledge and/or experience. Search terms included autism (``ASD'', ``ASD symptoms'', ``autism spectrum disorder'', ``Aspergers'', ``neurodevelopmental disorders''), adult (``adults''), healthcare professional (``allied healthcare professionals''), knowledge (``knowledge about autism'', ``knowledge about ASD'') and experience (``experience of autism''). Boolean operators were applied, where similar terms with concepts were combined using Or, and concepts were combined using AND (Table 1). The searches were limited to full text, English-language publications. Reference lists of included studies were screened for further eligible studies. Eligibility criteria were pre-defined, and studies were included if they reported on HCPs from any discipline or clinical setting who worked with autistic adults. Discipline/healthcare settings included were ``medicine, nursing, physiotherapy, speech and language therapy and radiography''. Grey literature (e.g. theses, dissertations, reports and pre-prints) was excluded. Study designs included qualitative, quantitative or mixed-methods, peer-reviewed publications from 2013 - 2026, ensuring that the evidence reflected the updated, Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) which was published in 2013 (American Psychiatric Association, 2013).
Table 1. Key search terms
| “Autism” or “ASD” or “ASD symptoms” or “autism spectrum disorder” or “Aspergers” or “neurodevelopmental disorders” and |
|---|
| “Adult” or “adults” and |
| “Healthcare professionals” or “allied healthcare professionals” or “healthcare workers” and |
| “Knowledge” or “knowledge about autism” or “knowledge about ASD” and |
| “Experience” or “experience of autism” |
2.3. Study selection
Identified articles from the search were exported into Covidence (Covidence, 2023), and duplicates were removed. Dual screening was carried out, and all voting was blinded. Titles and abstracts were independently screened by F.R. and M.G. against the inclusion criteria and labelled as ``yes'', ``no'', or ``maybe''. Inter-rater agreement at the title and abstract stage was 82%. Where there were conflicts or disagreements that could not be resolved, S.K. and M.M. acted as independent reviewers to make the final screening decision. F.R. then conducted a full-text review of all included studies against the inclusion criteria which was verified by a second reviewer (M.G.). Studies that partially met the criteria were discussed with the review team, and the final decisions were reached by group consensus. Data extraction for the final sample of studies was completed using a modified data extraction table created following guidance outlined in the Covidence data extraction template (Covidence, 2023). Data extraction was conducted by F.R. and cross-checked for accuracy and completeness by M.G. Extracted data included from the studies specified the name of the author(s), publication year, country, study design, study aim, data collection methods, sample and setting, and summary of key findings (see Table 2).
2.4. Data synthesis
A narrative synthesis was conducted to summarise the key characteristics of the included studies. F.R. carried out the analysis independently to gain an understanding of the themes that emerged. A meta-analysis was not feasible due to considerable variation in the outcome measures and assessment tools used to evaluate knowledge across studies. Therefore, an adapted CanMEDS competency framework was used to guide the data synthesis and organisation of findings. This framework enabled the categorisation of results relating to HCPs' knowledge and experiences of caring for autistic adults across multiple domains of healthcare competence.
2.5. Operational definitions
For the purpose of this review, key terms were operationally defined to ensure consistency in study selection and interpretation. Knowledge: HCPs' knowledge was defined as factual and self-perceived understanding of autism, including core characteristics, associations, communication needs and co-occurring conditions relevant to healthcare. Experience: Experience was defined as HCPs' frequency of direct clinical contact and self-reported exposure in caring for autistic adults during their professional practice. Training: To allow for the systematic examination of both the existing education provision and reported gaps in education, training was conceptualised as ``training received'' and ``training needs''. Training received was defined as any autism-specific education previously undertaken, including formal and informal education. Training needs were defined as HCPs' self-identified areas where additional autism-specific education or skill development was required to support effective care. While presenting the constructs as analytically distinct, it is acknowledged that the studies selected demonstrate conceptual overlap between knowledge, experience, and training. Clinical experience can function as an informal source of knowledge acquisition and training interventions are designed to influence both knowledge and practical competence. To support an integrated interpretation of the findings, the CanMEDS competency framework was used as an interpretive lens, viewing knowledge, experience and training as inter-related components of clinical competence.
2.6. Quality review
The Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018) was used to appraise the quality of all included studies (see Table 3). Quality appraisal was conducted independently by F.R., with a subset (30%) reviewed by M.G. Agreement was high, and discrepancies resolved through discussion. Across the quantitative studies, research questions were generally clearly stated and aligned with the data collected. Most studies employed appropriate measurement tools and statistical analyses relevant to their stated objectives (Alaghband-rad et al., 2023; Cashin et al., 2022; Eray & Murat, 2017; Gerçek et al., 2024; Malow et al., 2025; Micai et al., 2021; Ryan et al., 2022; Tromans et al., 2019; Shawahna et al., 2021;Watson-Grace et al., 2026; Zeleke et al., 2021). However, methodological limitations identified through quality appraisal reduce confidence in study conclusions, particularly in relation to training interventions where evidence should be interpreted as potential rather than definitive effectiveness due small sample size and inconsistent measurement tools. Several methodological limitations were identified, in particular, sample representativeness and potential response bias were frequently unclear or insufficiently reported in 21% of the studies (Alaghband-rad et al., 2023; Carlier et al., 2023; Gerçek et al., 2924; Zeleke et al., 2021). Additionally, aspects of sampling strategy were not consistently addressed in 10.54% of the studies, limiting the extent to which findings may be generalised (Alaghband-rad et al.; 2024, Zeleke et al. 2021). The mixed-methods studies included typically provided a clear rationale for the use of a mixed methods approach, although in 10.53% it was difficult to ascertain if there was adequate rationale for a mixed-methods approach (Mazurek et al. 2020; Stogiannos et al., 2021). Qualitative components were generally appropriate to the study aims, with data collection methods judged to be suitable in most cases; however, in 21% of the studies it was difficult to determine if inconstancies were addressed (Dillenburger et al., 2016; Edwards et al., 2025; Mazurek et al., 2020). One qualitative study met all MMAT criteria, demonstrating strong methodological coherence with appropriate data collection and analytical approaches clearly aligned to the study aims (Watson-Grace et al., 2026).
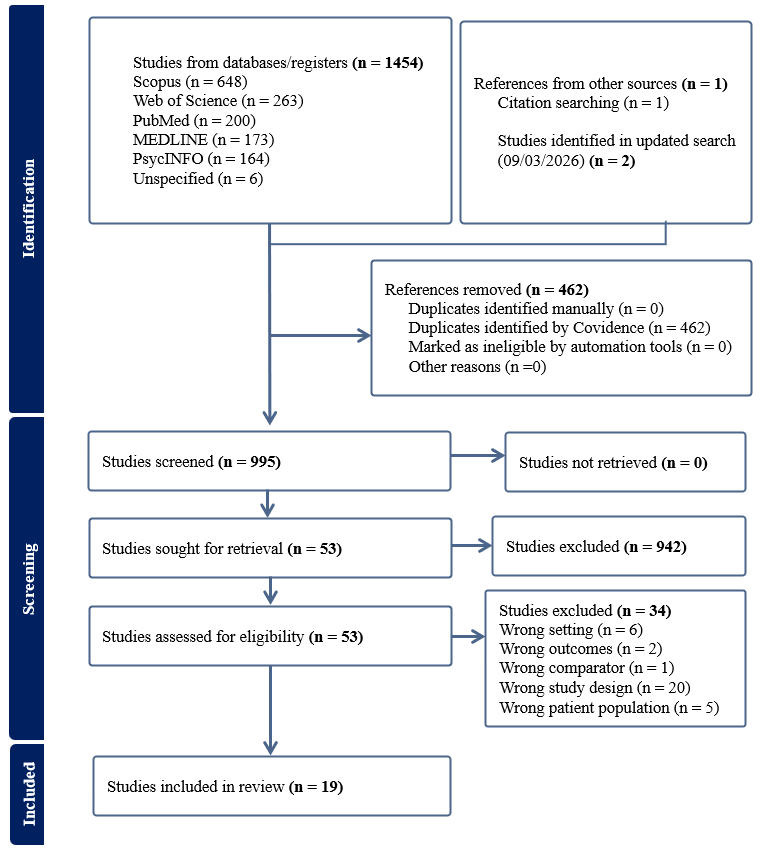
Table 2. Study Characteristics
| textbf{Author | Year} | Country | Study design | Study aim | Data collection | textbf{Sample | setting} | Summary of key findings |
|---|---|---|---|---|---|---|---|---|
| Watson-Grace et al., (2026) | USA | Qualitative exploratory design | Characterising nurses' perspectives on factors that influence their ability to provide patient-centred care for autistic adults in a large urban hospital system in the midwestern U.S. | Semi-structured interviews | Nurses- large urban hospital system (n= 12) | textbullet{} Most autism knowledge came from patient care rather than formal training. | ||
| textbullet{} Lack of formal autism-specific education at entry level nursing curriculum and employment related training. | ||||||||
| textbullet{} Experienced nurses reported autism was not covered in nursing school. | ||||||||
| textbullet{} Nurses with <5 years’ experience described inadequate autism education in their degree programs. | ||||||||
| textbullet{} Data suggests nurses must fill their own knowledge gaps. | ||||||||
| textbullet{} No participant mentioned employer-driven formal training. | ||||||||
| textbullet{} Multiple participants were unsure whether hospital education resources included autism specific. | ||||||||
| Edwards et al., (2025) | Australia | Mixed-methods cross-sectional online survey. | To assess autism-related knowledge, self-efficacy and disability attitudes, explore how these vary by demographic and professional factors and identify perceived challenges, effective strategies and support needs. | Modified Knowledge of Autism Scale (Unigwe et al., 2017) | Eye-care professionals (n=198) | textbullet{} Moderate-high self-efficacy (M= 23.05/30, SD=4.35) and autism knowledge (M=13.03, SD= 1.32). | ||
| AASPIRE Adult Autism Healthcare Provider Self-Efficacy Scale (Nicolaidis et al., 2021) | (Optometrists, Ophthalmologists, Certified Ophthalmic assistant, Ophthalmic technician, Optical dispenser Orthoptist, Eye clinic nurse) | textbullet{} More frequent interactions with autistic patients associated with greater self-efficacy. (p=0.001). | ||||||
| Attitudes and Perspectives towards Persons with Disabilities (Myong et al., 2021) | textbullet{} Majority reported training and system support needs (n=122). | |||||||
| textbullet{} Only 14% had received formal autism training. | ||||||||
| textbullet{} Participants represented 12 countries (Australia, UK, USA, Canada, New Zealand, Brazil Singapore, India, Italy, Ireland, Netherlands, Malta). | ||||||||
| Gerçek et al., (2024) | Turkey | Cross-sectional descriptive survey | To evaluate the knowledge level of ASD in healthcare workers from different occupational groups and the factors affecting the level of knowledge. | Knowledge about childhood autism among health workers questionnaire (KCAHW) | 317 healthcare professionals | textbullet{} Mean autism knowledge score: 12.62/19 (SD=2.807). | ||
| textbullet{} Highest knowledge area: deterioration in social interaction and communication (77.7%). | ||||||||
| textbullet{} Lowest knowledge area: co-occurring conditions (50.8%). | ||||||||
| textbullet{} Older HCPs had higher autism knowledge (r=0.139, p=0.013). | ||||||||
| textbullet{} 50.2% reported receiving no autism training. | ||||||||
| textbullet{} 63.3% of doctors had autism-specific training. | ||||||||
| Alaghband-rad et al., (2023) | Iran | Cross-sectional survey | To assess the knowledge, attitudes and practice of healthcare providers for patients with adult autism and to determine the needs of healthcare staff to provide convenient care to autistic adult patients. | Two-part questionnaire: - Demographics | 182 healthcare professionals (Mental health professionals, general physicians, others) | textbullet{} 69.2% - knowledge poor or fair. | ||
| -Questions 1 to 6, and question 8 of questionnaire used in Zerbo et al (2015) study. | textbullet{} 10% excellent or very good. | |||||||
| textbullet{} 64.8% reported needing training on effective communication strategies. | ||||||||
| textbullet{} Lack of knowledge | preparedness for adult autism remains a key barrier to service provision. | |||||||
| Carlier et al., (2023) | Switzerland | Qualitative, exploratory design. | To explore and understand the strategies used by radiographers to image autistic patients in Swiss medical imaging departments, highlight enablers and challenges and offer some respective recommendations, adapted to the Swiss service provision. | Semi-structured interviews | 100 radiographers (radiographer practitioner, research, manager, educator, modality superintendent, radiation protection expert | chief radiographers) | textbullet{} 60% had previously managed an autistic patient. | |
| textbullet{} 3% reported practical lived experience. | ||||||||
| textbullet{} Training needs identified: | ||||||||
| 1. Communication with autistic patient | their carers (46%) | |||||||
| 2. Understanding autistic patients’ needs (76%) | ||||||||
| 3. Calming the patient (71%) | ||||||||
| 4. Recognising autistic patients (63%) | ||||||||
| · Training received: | ||||||||
| 1. Specific autism training: 3% | ||||||||
| 2. Short term training: 2% | ||||||||
| 3. Lecture @ Bachelor’s level: 1% | ||||||||
| Malow et al., (2023) | USA | Pre-post intervention pilot study | To determine whether participation in the ECHO Autism Transition training increased primary care providers’ confidence in caring for autistic adults. | Self-report surveys (pre | post intervention) | Primary care physicians (cohort 1 n=20), cohort 2 n=17) | Self-efficacy: | |
| Knowledge assessment questionnaire developed specifically for the study. | · Cohort 1: Increased 18.9 - 20.3, significant (t= -1.855, p= 0.042). | |||||||
| · Cohort 2: Increased 20.5-23.1, not significant (t= -1.721, p=0.058). | ||||||||
| · PCASE (Cohort 2): Improved 179.4 (SD 57.4) - 222.2 (SD 34.0), significant (t= -3.423, p= 0.003). | ||||||||
| Knowledge: | ||||||||
| · Cohort 1: Increased 20.1 (SD 2.7) - 21.0 (SD 2.0), not significant (t= -1.464, p= 0.083). | ||||||||
| · Cohort 2: Increased 18.9 (SD 2.4) - 20.6 (SD 2.1), significant (t= -3.50, p=0.003). | ||||||||
| Cashin et al., (2022) | Australia | Cross-sectional descriptive survey | To contribute to filling identified gaps in literature by surveying registered nurses in mainstream hospital and community-based healthcare settings nationally in relation to self-reported knowledge, preparedness, comfort, and confidence in caring for people with Intellectual Disability (ID) and/or autism. | Self-designed (with content validation.) | 693 registered nurses. | textbullet{} 55.7% felt somewhat knowledgeable about co-occurring conditions and care issues in ID/autism. | ||
| textbullet{} 7.1 specialist nurses reported contact with people with an ID and/or autism. | ||||||||
| textbullet{} Postgraduate education: | ||||||||
| - Fornal postgraduate training in ID/autism: 7.6% | ||||||||
| - Graduate certificate: 4.3% | ||||||||
| - Graduate diploma: 2.3% | ||||||||
| - Master’s degree: 0.9% | ||||||||
| - Doctorate-:0.1% | ||||||||
| Ryan et al., (2022) | USA | Pre-post educational intervention (single group) | To evaluate whether an interdisciplinary training program improved trainee’s knowledge about autism. | 1. The Autism Spectrum Knowledge Scale Professional Version (ASKSP). | 170 interdisciplinary trainees. - | textbullet{} Measured knowledge (ASKSP) - Pre-LEND M=28.2, 85.4%, SD 2.41) Post-LEND (M=29.0, 87.9%, SD =2.51). | ||
| 2. Perceived autism spectrum disorder knowledge. | Applied behaviour analysis, Audiology *Dentistry *Education *Family advocates Genetics *Health-care administration *Legal *Medicine *Neuroscience *Nursing *Nutrition *Occupational Therapy *Paediatrics *Physical therapy *Psychology *Public Health *Social work *Special education *Speech | language pathology | textbullet{} Self-perceived ASD knowledge: Pre-LEND M=59.8, SD= 18.5) - Post-LEND M=79.7, SD =11.3. | |||||
| 3. Self-reported confidence. | textbullet{} Self-reported confidence: Pre-LEND M=58.0, SD=21.6 - Post-LEND (M=78.0, SD=13.2) | |||||||
| 4. Training experiences - self reported. | ||||||||
| Stogiannos et al., (2021) | UK | Cross-sectional survey with mixed methods | To explore the perspectives of UK radiographers in relation to MRI scanning of autistic individuals, to map out their current knowledge and understanding in relation to autism, to understand radiographic practices | approaches used, and to identify potential training needs. | Specifically designed mixed-methods questionnaire - not validated. | 130 radiographers | textbullet{} Knowledge needs: | |
| Understanding patients’ needs (90%); recognising autistic patients (70%); optimal communication with patients (88%) | ||||||||
| textbullet{} Experience: 86.8% had scanned an autistic patient; 93.7% had prior positioning/scanning experience. | ||||||||
| textbullet{} Training: 75.6% received no training on autism; 10% received formal university training ;10% online training; 30% attended a short course; 20% received mandatory training at the hospital | ||||||||
| 30% reported “other” forms of training. | ||||||||
| Zeleke et al., (2021) | Ethiopia | Single group, pre-post design | To measure the effectiveness of autism training provided to help professionals in Ethiopia. | Self-created autism knowledge assessment test. | 34 healthcare professionals | textbullet{} Pre - post training improvements: | ||
| -Understanding autism symptoms: 2.2 (SD1.0) - 4.6 (SD0.78) | ||||||||
| - Understanding the nature of autism: 2.0 (SD 1.15) - 4.7 (SD 0.49) | ||||||||
| - Understanding cause and associated factors: 0.87 (SD 0.63) - 1.8 (SD 0.42) | ||||||||
| Micai et al., (2021) | Denmark | Cross-sectional online survey | To explore the experiences and perceptions by autistic adults, carers of autistic adults and adult service professionals on psychiatric and medical co-occurring conditions and health behaviours in autistic adults. | Separate versions of the ASDEU online survey were developed for the 3 target groups. | In the health-section; 113 were healthcare professionals | |||
| textbullet{} 51% believed that poor adherence to treatment for an already diagnosed condition contributed to hospital contact. | ||||||||
| textbullet{} 65% believed late recognition of a health problem contributed to hospital contact. | ||||||||
| textbullet{} Identified knowledge gaps regarding autism-related health risks, highlighting the need for improved professional training. | ||||||||
| Shawahna (2021) | Palestine | Cross-sectional survey | 1.) Assess self-rated familiarity of practicing nurses in Palestine regarding autism. | Specifically designed questionnaire - not validated | 357 registered nurses | textbullet{} . 46% completed autism-related courses in their degree. | ||
| 2.) Assess self-rated confidence of practicing nurses in Palestine in their abilities to provide counselling for parents/family/caregivers on the drugs prescribed for children/patients with ASDs and their potential adverse effect. | textbullet{} 17.9% completed continuing educational course/program. | |||||||
| 3.) Assess willingness of practicing nurses in Palestine to receive education/training on issues in autism. | textbullet{} Nurses with ≥7 years’ experience had higher familiarity scores (M= 38.2, SD=19.6) than those with ≤7 years (M=32.6, SD=17.5, p= 0.006) | |||||||
| 4.) Identify the sociodemographic and practice variables that could predict high self-rated familiarity scores. | textbullet{} Nurses with a Master’s / postgraduate degree scored higher mean familiarity scores of 41.9 (SD=20.4), compared to nurses with a bachelor’s degree (M=34.6, SD=20.4) - (p=0,007). | |||||||
| textbullet{} Nurses who completed autism related courses during their nursing degree scored higher (M=37.5, SD=17.5) than those without autism related courses (M=33.8, SD=20.4) - (p=0.0064). | ||||||||
| textbullet{} Continuing education showed the strongest effect (p < 0.001), with a small-moderate positive correlation (r = 0.21). | ||||||||
| Mazurek et al., (2020) | USA | Pre-post intervention pilot study | To determine whether participation in the ECHO Autism Transition training increased primary care providers’ confidence in caring for adolescents and young adults with autism. | 12 Primary care physicians | textbullet{} Knowledge scores: Improved from 67.3% (SD 11.5) to 71.9% (SD 12.6); not statistically significant (Z = -1.79, p = .074). | |||
| Pre and post training questionnaires (designed specifically to measure self-efficacy, knowledge and practice). | textbullet{} Prior training: 56% had previous autism training. | |||||||
| 1 hour videoconferencing session. | textbullet{} Implication: Training recommended across disciplines to enhance coordinated care. | |||||||
| Post program evaluation surveys. | ||||||||
| Urbanowicz et al., (2020) | Australia | Cross-sectional online survey | To describe the experiences, views, and needs of Australian health professionals providing care to adults on the autism spectrum. | Specifically designed online survey - not validated. | 78 health professionals commonly working as medical practitioners, nurses, or occupational therapists. | textbullet{} Training occurred during one or more of the following: 1. accumulative clinical experience (60%) 2. On-the-job training (58%) | ||
| Questions describing adult patients with autism | training needs of HCP adapted from research conducted by Bruder et al (2012) | 3. Professional education (44%) | ||||||
| 4. Self-learning (48%) | ||||||||
| 5. Undergraduate or postgraduate study (23%). | ||||||||
| Tromans et al., (2019) | UK | Cross-sectional survey | Primary aim: To explore the perspectives of Intellectual Disability healthcare professionals regarding autism in adult females. | Self-created questionnaire | 80 Intellectual disability healthcare professionals | textbullet{} 33% received formal training for autism diagnosis. | ||
| Secondary aim: To collect information pertaining to Intellectual Disability healthcare professionals’ perceived autism related training needs. | textbullet{} 76% reported having autism-related training needs. | |||||||
| textbf{Eray | Murat (2017)} | Turkey | Single group, pre-post design | Determining the level of knowledge of family practitioners regarding ASD. | Study specific survey - not standardised or validated. | 75 Family practitioners | textbullet{} Sufficient autism information: Increased from 34.7% pre‑training to 88% post‑training. | |
| Questionnaire consisted of 6 questions, including sub-items about general knowledge about autism and demographic information | textbullet{} Belief that autism always involves intellectual disability: Decreased from 40% to 17.3% post training. | |||||||
| textbullet{} Belief that eye contact excludes autism: Decreased from 29.3% to 24% post training. | ||||||||
| Havercamp et al., (2016) | USA | Mixed- methods; survey | follow up panel discussions. | To determine the effectiveness of autism training for medical students. | Medical student survey | 99 third year medical students | textbullet{} 68.7% cited the experience allowed them to learn more about autism in general. | |
| A panel discussion with professionals, people with autism and family members on the healthcare needs of autistic children and adults. | textbullet{} 28.3% cited having a better understanding of autism. | |||||||
| Dillenburger et al., (2016) | UK / NI | Non-comparative, cross sectional | To examine post-qualifying autism training for professionals by exploring knowledge, training and practical experiences of health, social care and educational staff working across autism-related settings. | Researcher designed survey, based on the Professional Autism Needs Questionnaire (PAN-Q) - not standardised or validated. | 569 health | social care staff | textbullet{} Post-qualifying autism training: 29% received basic in-service training. | |
| textbullet{} Training levels completed: 12% level 1; 10% level 2; 3% level 3. | ||||||||
| textbullet{} Support needs: Some respondents felt access to a designated autism “expert” would be helpful. | ||||||||
| textbullet{} Training recommendations: Majority recommended incorporating autism training into professional education or staff induction. | ||||||||
| Zerbo et al., (2015) | USA | Mixed methods Questionnaire | interviews | To determine healthcare providers’ general knowledge about autism, to assess their comfort level treating autistic patients. | Specifically designed survey - not standardised or validated but pilot tested among members of the Autism in Adults Workgroup and tested for readability and completion time. | 922 healthcare providers completed the online survey. | textbullet{} Self-rated knowledge/skills: 30% poor, ~50% fair, <10% excellent. | |
| textbullet{} Autistic patients on caseload: ~20% had 1-5, ~30% had 6-10, ~50% had >10. | ||||||||
| Follow-up interviews | 9 primary care physicians were interviewed. | textbullet{} Training needs: Most frequently endorsed need was training in effective communication with autistic patients. | ||||||
| textbullet{} Service suggestions: Some physicians recommended dedicated multidisciplinary clinics for autistic adults. |
3. Results
Analysis focused on knowledge, experience, and training, including training provision and identified needs.
3.1. Knowledge
Across six pre-post intervention studies, training was consistently associated with improvements in autism-related knowledge, although the extent of improvement varied depending on whether knowledge was measured objectively or by self-report Eray & Murat, 2012; Havercamp et al., 2016; Mallow et al., 2023; Mazurek et al., 2020; Ryan et al., 2022; Zeleke et al., 2021;). Improvements were observed in both objective knowledge scores, for example, absolute increases +1.7 [18.9 to 20.6] after a 12-week programme (Malow et al., 2023) and +0.8 points (28.2 - 29.0) among interdisciplinary trainees as well as self - perceived knowledge increases such as +20.8 points (58.9 - 79.7) (Ryan et al., 2022). Collectively, these findings suggest that structured training may improve autism-related knowledge across a range of HCPs and healthcare setting; however, direct comparison across studies is limited by heterogeneity in knowledge assessments and reporting, which prevented the calculation of pooled effect estimates. In contrast, four non-intervention studies that assessed knowledge at a single time point demonstrated a consistent pattern of low-to-moderate perceived autism knowledge among HCPs, with substantial proportions rating their knowledge as poor/fair and few reporting high confidence (Alaghband-rad et al., 2023; Gerçek et al.,2024; Stogiannos et al., 2021; Zerbo et al., 2015). Where objective tools were used, such as the Knowledge about Childhood Autism among Health Workers (KCAHW), average scores suggested only moderate knowledge (Gerçek et al., 2024). Overall, the cross-sectional evidence indicates that baseline autism knowledge remains variable and frequently limited in routine HCP practice (Corden et al., 2022). These deficits are clinically consequential as limited understanding of co-occurring conditions may contribute to misattribution of mental health or medical symptoms, consistent with diagnostic overshadowing (Hamdan et al., 2024; Strömberg et al., 2022), while communication-related gaps may underpin a broader mismatch between HCPs and autistic adult patients (Malik-Soni et al., 2022; Mason et al., 2021; Nicolaidis et al., 2015). By profession, perceived knowledge tended to be higher among HCPs reporting more frequent contact with autistic adult patients (Cashin et al., 2022; Urbanowicz et al., 2020). This is evidenced by physicians and radiographers frequently reporting knowledge gaps despite clinical experience (Carlier et al., 2023; Zerbo et al., 2015), while nurses and interdisciplinary trainees commonly reported limited formal preparation and relied on informal learning (Cashin et al. 2022; Ryan et al., 2022). Overall, the knowledge evidence supports a need for training that moves beyond general awareness toward competency-based content. When interpreted through the CanMEDS framework, these findings relate primarily to gaps within the ``medical expert role'' (autism-specific clinical knowledge, including co-occurring conditions) and ``communicator role'' (knowledge to support effective communication accommodation). Additionally, the variable awareness of evolving evidence and limited indication of ongoing professional development also aligns with challenges within the ``scholar role''.
3.2. Experience
Across studies, clinical experience with autistic adult patients varied greatly by role and country. Reported experience ranged from very limited experience (7.1% among specialist intellectual disability nurses in Australia) to widespread experience in other settings (93.7% for UK radiographers) (Cashin et al., 2022; Stogiannos et al., 2021). By profession, experience was most consistently reported among radiographers and primary care physicians, reflecting routine clinical contact in imaging and general practice (Carlier et al., 2023; Stogiannos et al., 2021; Zerbo et al., 2015), whereas specialist intellectual disability nursing cohorts reported lower proportions of routine experience in some settings (Cashin et al., 2022). Across professions, greater experience was generally associated with higher perceived self-efficacy, suggesting experience may support practical adaptation of care processes in healthcare settings. By country, experience patterns differed even within the same profession. For example, radiographers reported greater experience in the UK compared with Switzerland, indicating that local service pathways (Carlier et al., 2023; Stogiannos et al., 2021). Another cross-study pattern was that limited experience itself was frequently cited as a barrier to delivering appropriate care, whereas greater experience with autistic adults was associated with higher perceived self-efficacy (Edwards et al., 2025; Urbanowicz et al., 2020). In Urbanowicz et al., (2020), HCPs working in disability or autism-specific settings reported higher perceived competence in providing care than those working outside these settings, suggesting that routine experience may shape confidence as well as skill development. Edwards et al., (2025) similarly reported that more frequent clinical contact with autistic patients predicted higher clinician self-efficacy, indicating that repeated experience may support the development of strategies for reasonable adjustments and adaptations. However, as these outcomes are generally self-reported and often resulting from cross-sectional designs, these should be interpreted as indicative of an association rather than evidence of an effect. Taken together, these findings suggest that experience functions as a potential mechanism through which HCPs develop practical competence in adapting assessment, communication, and procedures for autistic adult patients, particularly in time-pressured healthcare settings. Interpreted through CanMEDS, these patterns align with the ``medical expert role'' (practice-based development of clinical judgement and procedural adaptation) and have implications for the ``communicator role'' as experience may support the development of tailored communication strategies and reasonable accommodations.
4. Training
4.1. Training received by healthcare professionals
Across studies, autism-specific training was inconsistent and often limited, with clear variation across professions, countries and training pathways. By profession, training exposure appeared uneven. Physicians more commonly reported some prior autism-specific training, often distributed across medical school, residency and short courses, whereas radiographers and intellectual disability HCPs reported particularly low levels of autism-specific training, frequently relying on ``on-the-job'' learning. By country, access to training varied markedly, ranging from relatively higher levels (63%) among Turkish doctors (Gerçek et al.,2024) to very low levels (15%) among Ethiopian HCPs (Zeleke et al., 2021), indicating substantial inequity in access to autism-specific education. A recurring cross-study pattern was informal, experiential learning rather than structured education. Australian HCPs more commonly reported informal learning (58%) and comparatively few reported receiving (23%) autism-specific content during undergraduate or postgraduate education (Urbanowicz et al., 2020). This was similar in the United Kingdom (UK) / Northern Ireland (NI), with a minority (29%) of HCPs reporting any autism training, most of which were brief awareness sessions (Dillenburger et al., 2016), suggesting limited depth and coverage of applied competencies. Training exposure appeared higher during initial qualification for Palestinian nurses (54.6%), whereas formal postgraduate autism-specific training was notably low (7.6%) in Australian nurses (Cashin et al., 2022; Shawahna et al., 2021). Among US primary care physicians, over half (56.6%) reported previous autism training, although the extent varied over medical school, residency and short courses (Mazurek et al., 2020). Radiographers' training was also low with only 3% in Switzerland reporting specific autism training (Carlier et al.,2022), compared to higher but inconsistent levels among UK radiographers (Stogiannos et al., 2021), indicating that even within a single profession, training may depend heavily on local service priorities and opportunities (Carlier et al., 2022; Stogiannos et al., 2021). There were similar gaps in other professions, including only 33% of intellectual disability HCPs, reinforcing that autism-specific training is not routinely embedded across disciplines (Tromans et al., 2019). Within the CanMEDS framework, the pattern of limited and irregular training aligns with gaps in the ``scholar role'', specifically the acquisition and application of knowledge and suggests that key competencies may not be systematically developed across professional education or CPD pathways. Overall, the limited scope of training identified suggests these competencies may not be adequately addressed. Training needs of healthcare professionals The most frequently identified need across all countries was communication. By profession, communication and interaction adjustments were consistently prioritised, including among radiographers and primary care physicians (Alaghband-rad et al., 2023; Carlier et al., 2023; Zerbo et al., 2015). HCP needs also extended to recognising autism in adults, managing sensory sensitivities, and adapting routine clinical processes (Alaghband-rad et al., 2023; Carlier et al., 2023; Edwards et al., 2925; Gerçek et al., 2024; Micai et al., 2021; Tromans et al., 2019; Zerbo et al., 2015). By country, communication remained a dominant theme, including in countries such as Iran, Switzerland, the US, and the UK, however, emphasis varied with other priorities stated as screening tools and recognition, continuing education access and workplace-based training (Alaghband-rad et al., 2023; Carlier et al., 2023; Dillenburger et al., 2016; Tromans et al., 2019; Zerbo et al., 2015). In Iran, HCP prioritised training in communication strategies (64.8%) and screening tools (60.4%) (Alaghband-rad et al., 2023). Similarly, Swiss radiographers also emphasised communication with autistic adult patients and their carers (Carlier et al., 2023), along with 70.8% of US physicians (Zerbo et al., 2015). Radiographers in the UK reported substantial training needs in understanding (90%), communication (88%) and autism recognition (70%) (Stogiannos et al., 2021). Other studies highlighted broader educational gaps, including Palestinian nurses' need for continuing education (Shawahna et al., 2021) and HCPs' limited understanding of health risks associated with autistic adults (Micai et al., 2021). More recent findings also point to deficits in both entry-level education and in employment-related training (Watson-Grace et al., 2026). When mapped to the CanMEDS framework, these needs extend beyond the ``medical expert role'' and highlight gaps in the ``communicator role'', especially in relation to adapting interactions to meet the needs of autistic adults.
Table 3. MMAT Quality Assessment
| First author and Year | Clear research questions | Data addresses research questions | 1.1 Qualitative approach appropriate | 1.2 Adequate data collection methods | 1.3 Sampling methods appropriate | 1.4 Finding adequately derived from data | 1.5 Interpretation sufficiently substantiated | 1.6 Coherence between data, analysis, interpretation | 2.1 Relevant sampling strategy | 2.2 Representative sample | 2.3 Appropriate measurements | 2.4 Low risk of response bias | 2.5 Appropriate statistical analysis | 3.1 Adequate rationale for mixed methods | 3.2 Effectively integrated components | 3.3 Outputs adequately interpreted | 3.4 Inconsistencies addressed | 3.5 Meets criteria for both components |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Articles reporting quantitative data | ||||||||||||||||||
| Eray (2017) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Tromans (2019) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Zeleke (2021) | Y | Y | N | N | N | Y | Y | |||||||||||
| Shawahna (2021) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Micai (2021) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Cashin (2022) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Ryan (2022) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Alaghband-rad (2023) | Y | Y | Y | N | Y | CT | Y | |||||||||||
| Mallow (2023) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Gerçek (2024) | Y | Y | Y | Y | Y | CT | Y | |||||||||||
| Articles reporting both quantitative and qualitative data (mixed methods) | ||||||||||||||||||
| Zerbo (2015) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Dillenburger (2016) | N | Y | Y | Y | Y | CT | Y | |||||||||||
| Havercamp (2016) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Urbanowicz (2020) | Y | Y | Y | Y | Y | Y | Y | |||||||||||
| Mazurek (2020) | Y | Y | CT | Y | Y | CT | Y | |||||||||||
| Stogiannos (2021) | Y | Y | C T | Y | Y | CT | Y | |||||||||||
| Carlier (2023) | Y | Y | Y | Y | Y | CT | CT | |||||||||||
| Edwards (2025) | Y | Y | Y | Y | Y | CT | Y | |||||||||||
| Articles reporting qualitative data | ||||||||||||||||||
| Watson-Grace (2026) | Y | Y | Y | Y | Y | Y | Y | Y | ||||||||||
Note. Y = Yes, N = No, CT = Can't tell
5. Discussion
This review highlights that gaps in autism-specific education and training directly influence HCPs' clinical interactions with autistic adults. While some HCPs reported having some baseline knowledge, its accuracy and depth varied, influencing their ability to recognise co-occurring conditions and provide appropriate care (Corden et al., 2022, Doherty et al., 2021, Sala et al., 2020). Variability across studies may partly reflect differences in measurement, particularly with self-assessment tools. Although pre-post studies demonstrated potential knowledge gains, improvements were inconsistent, likely reflecting heterogeneity in intervention content. The widespread use of non-standardised, non-validated tools, small sample sizes and lack of control groups further limits comparability across studies. In addition, many studies relied on self-reported knowledge, which may not accurately reflect objective competence and influenced by social desirability. Potential publication bias should be considered when interpreting these findings as positive training outcomes may be preferentially published. The generalisability is limited by substantial heterogeneity across studies, including differences in countries, healthcare systems, professional roles, clinical settings, and baseline experience with autistic adults. Collectively, these factors mean findings should be interpreted as indicative of potential patterns rather than definitive estimates of knowledge levels or training effectiveness across the wider HCP population. Experience emerged as a distinct component of competence. Studies suggested that greater experience with autistic adults was associated with higher perceived self-efficacy, whereas limited experience was frequently reported as a barrier to providing appropriate and effective care (Edwards et al., 2025, Urbanowicz et al., 2020). In practice, the type of experience differed by profession, for example, procedural, time-limited encounters with radiographers may require different communication and sensory accommodations compared to primary care physicians contact involving broader recognition and management of co-occurring conditions. Overall, the variation in clinical experience suggests that competence in autism-specific care is multi-dimensional and encompasses not only what HCPs know, but also how effectively they can apply adjustments. The application of the CanMEDS framework allowed for a broader interpretation of findings beyond knowledge deficits alone, highlighting competency gaps across multiple domains. While limited autism-specific knowledge was frequently emphasised, mapping these findings to CanMEDS highlights that deficits extend beyond the ``medical expert role'' and include the ``communicator'', ``health advocate'', and ``professional roles''. In particular, challenges in adapting communication styles to meet autistic adults' needs, diagnostic overshadowing with misattribution of symptoms to autism rather than co-occurring conditions, understanding sensory barriers affecting care environments and procedures all suggest persistent gaps in communication-related competencies. Similarly, the limited ability to address systemic barriers and advocate for appropriate adjustments reflects deficits within the ``health advocate role''. These deficits extend beyond knowledge alone and reflect broader systemic and competency-related gaps. Training interventions produced mixed outcomes, underscoring the absence of standardised educational approaches and the need for systematic integration of autism content within healthcare curricula (Malik-Son et al., 2020). These findings suggest that current training approaches may be insufficient to support the development of holistic competence in autism care. At policy level, these disparities point to national-level differences in training expectations. Autism-specific training was consistently limited across countries and professions and when training was available, it was typically delivered through short courses, mandatory hospital training, or online modules (Carlier et al., 2023; Cashin et al., 2022; Dillenburger et al., 2916; Edwards et al., 2025; Havercamp et al., 2026; Shawahna, 2021; Stogiannos et al., 2021; Tromans et al., 2019; Urbanowicz et al., 2020). Very few HCPs received formal education, which may account for the existing knowledge gaps. The absence of formal autism content in undergraduate curricula and a lack of systematic continuing professional development opportunities was identified throughout the literature (Carier et al., 2023, Cashin et al., 2022, Shawahna, 2021). HCPs also reported a need for access to autism specialists or specialist clinics (Alaghband-rad et al., 2023; Dillenburger et al., 2016; Malow et al., 2023; Mazurek et al., 2020; Stogiannos et al., 2021; Zerbo et al., 2015). While specialist input is valuable, it does not replace the need for frontline HCPs to attain a baseline level of autism competence. A competency-based approach to education, aligned with frameworks such as CanMEDS, may better address the complex and multi-dimensional skills required to care for autistic adults. This includes the acquisition of knowledge, as well as the development of practical communication skills, interprofessional collaboration, and advocacy capabilities. Strengths and limitations This review employed a comprehensive search strategy and rigorous quality appraisal of all included studies. There was substantial heterogeneity in participant demographics, professional roles, and sample sizes, which limited the ability to draw definitive conclusions and reduced the generalisability of findings across settings and professions. The lack of standardised or validated tools to measure autism knowledge further affected comparability and prevented quantitative meta-analysis. In addition, many studies relied on self-reported knowledge, which may not accurately reflect objective competence and can be influenced by social desirability, particularly in pre-post designs. One study did not distinguish between child and adult autism despite using the KCAHW, reducing its relevance to adult-focused knowledge. Finally, restricting the review to English-language publications, and studies aligned with the review criteria may have introduced selection and reporting bias. Publication bias is also possible, as studies reporting positive findings may be more likely to be published than those reporting null or mixed results; formal assessment was not feasible given heterogeneity and the absence of pooled effect estimates. It is important to acknowledge that CanMEDS was originally developed within the context of physicians, and its application across a broader range of HCPs may not fully capture role-specific competencies. Additionally, not all findings fit neatly within predefined roles, suggesting potential limitations in applying a structured framework to heterogeneous evidence. Despite this, the framework provided a practical lens through which the gaps in practice could be conceptualised and helped identify priorities for training and professional development.
6. Conclusion
This review identified nineteen studies examining HCPs knowledge, experience, and training in relation to autistic adults. Despite substantial methodological and contextual variation, consistent patterns emerged that demonstrated limited autism-specific knowledge, variable clinical experience, and inconsistent training levels. These gaps were compounded by non-standardised assessment methods and the absence of validated knowledge measurement tools. While some educational interventions demonstrated short-term improvements, the impact was inconsistent and constrained by the lack of a standardised curriculum or training framework. Alongside these limitations, HCPs consistently reported unmet training needs, particularly in communication, identification of autistic adult patients, and the management of sensory and co-occurring health conditions. Collectively, these findings highlight a clear need for structured, evidence-based autism education embedded across undergraduate training and continuing professional development. A competency-based approach to training, aligned with frameworks such as CanMEDS, may support more consistent training/education by not only targeting knowledge acquisition, but also practical communication skills, person-centred adaptations, and advocacy for reasonable adjustments. Future research should prioritise the development and evaluation of standardised education frameworks and explore the meaningful involvement of autistic individuals in curriculum design and delivery to support more consistent, person-centred care. The authors declare no conflict of interest.
References
- Alaghband-rad, J and Ardeshir, M and Hakki Kazazi, E and Motamed, M (2022). Adult autism spectrum disorder: knowledge, attitude and practice of health system professionals. The Journal of Mental Health Training, Education and Practice, 18, 185-194. https://doi.org/10.1108/jmhtep-07-2022-0066
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed. , text rev.). https://doi.org/10.1176/appi.books.9780890425787.
- Bradshaw, P and Pellicano, E and van Driel, M and Urbanowicz, A (2019). How Can We Support the Healthcare Needs of Autistic Adults Without Intellectual Disability? Current Developmental Disorders Reports, 6(2), 45-56.
- Brugha, T. S and McManus, S and Bankart, J and Scott, F and Purdon, S and Smith, J and Bebbington, P and Jenkins, R and Meltzer, H (2011). Epidemiology of autism spectrum disorders in adults in the community in England.
- Carlier, S and Vorlet, P and C, S. D. R and Malamateniou, C (2023). Strategies, challenges and enabling factors when imaging autistic individuals in Swiss medical imaging departments. Journal of Medical Imaging and Radiation Sciences, 54. https://doi.org/10.1016/j.jmir.2022.11.002
- Cashin, A and Pracilio, A and Buckley, T and Kersten, M and Trollor, J and Morphet, J and Howie, V and Griffin, K and Wilson, N. J (2022). A survey of Registered Nurses' educational experiences and self-perceived capability to care for people with intellectual disability and/or autism spectrum disorder. Journal of Intellectual and Developmental Disabilities, 47, 227-239. https://doi.org/10.3109/13668250.2021.1967897
- Corden, K and Brewer, R and Cage, E (2022). A Systematic Review of Healthcare Professionals' Knowledge, Self-Efficacy and Attitudes Towards Working with Autistic People. Review Journal of Autism and Developmental Disorders, 9, 386-399. https://doi.org/10.1007/s40489-021-00263-w
- Dietz, P. M and Rose, C. E and McArthur, D and Maenner, M (2020). National and State Estimates of Adults with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 50, 4258-4266. https://doi.org/10.1007/s10803-020-04494-4
- Dillenburger, K and McKerr, L and Jordan, J. A and Keenan, M (2016). Staff Training in Autism: The One-Eyed Wo/Manet al.. International Journal of Environmental Research and Public Health, 13. https://doi.org/10.3390/ijerph13070716
- Doherty, M and Neilson, S and O'Sullivan, J and Carravallah, L and Johnson, M and Cullen, W and Shaw, S. C. K (2022). Barriers to healthcare and self-reported adverse outcomes for autistic adults: a cross-sectional study.
- Edwards, C and Love, A. M. A and Cai, R. Y and Constable, P. A and Love, D. C and Parmar, K and Gowen, E and Gibbs, V (2025). Autism in eye care: A mixed-methods study of professional knowledge, confidence and clinical experience.
- Eray, S and Murat, D (2017). Effectiveness of autism training programme: An example from Van, Turkey. Journal of Pakistan Medical Association, 67, 1708-1713.
- Frank, J. R and Snell, L and Sherbino, J. (Eds.) (2015). CanMEDS 2015 physician competency framework.
- Fyfe, C and Winell, H and Dougherty, J and Gutmann, D.H and Kolevzon, A and Marrus, N and Tedroff, K and Turner, T.N and L.A, Weiss and Yip, B.H.K and {Yin} and Sandin, S (2026). Time trends in the male to female ratio for autism incidence: population based, prospectively collected, birth cohort study.
- Unknown (2024). The level of knowledge about autism spectrum disorders among a university hospital healthcare professionals in Turkey. Journal of Clinical Psychiatry, 27, 12-20. https://doi.org/10.5505/kpd.2024.86836
- Hamdan, S. Z and Bennett, A (2024). Autism-Friendly Healthcare: A Narrative Review of the Literature.
- Havercamp, S. M and Ratliff-Schaub, K and Macho, P. N and Johnson, C. N and Bush, K. L and Souders, H. T (2016). Preparing Tomorrow's Doctors to Care for Patients with Autism Spectrum Disorder.
- Unknown (2018). The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for Information, 34(4), 285-291. https://doi.org/10.3233/efi-180221.
- Lai, M. C and Baron-Cohen, S (2015). Identifying the lost generation of adults with autism spectrum conditions.
- Malik-Soni, N and Shaker, A and Luck, H and Mullin, A. E and Wiley, R. E and Lewis, M. E. S and Fuentes, J and Frazier, T. W (2022). Tackling healthcare access barriers for individuals with autism from diagnosis to adulthood. Paediatric Research, 91(5), 1028-1035. https://doi.org/10.1038/s41390-021-01465-y.
- Malow, B. A and Mazurek, M and Stobbe, G and Agrawal, M. M and Loftin, R and Caudel, D and Hess, A and Westphal, A and Smith, J and Shouse, J and Cheak-Zamora, N and Sohl, K (2023). ECHO autism adult healthcare: Training community clinicians to provide quality care for autistic adults.
- Mazurek, M. O and Stobbe, G and Loftin, R and Malow, B. A and Agrawal, M. M and Tapia, M and Hess, A and Farmer, J and Cheak-Zamora, N and Kuhlthau, K and Sohl, K (2020). ECHO Autism Transition: Enhancing healthcare for adolescents and young adults with autism spectrum disorder.
- Unknown (2021). Autistic Adult Health and Professional Perceptions of It: Evidence from the ASDEU Project.
- Unknown (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.
- Rosen, T. E and Mazefsky, C. A and Vasa, R. A and Lerner, M. D (2018). Co-occurring psychiatric conditions in autism spectrum disorder. International Review of Psychiatry, 30(1), 40-61. https://doi.org/10.1080/09540261.2018.1450229.
- Ryan, T. D and Brunson McClain, M and Merrill, A and Dahir, N and Harris, B and Irby, S. M (2021). Preliminary investigation of interdisciplinary trainee's improvement in knowledge about autism spectrum disorder.
- Sala, R and Amet, L and Blagojevic-Stokic, N and Shattock, P and Whiteley, P (2020). Bridging the Gap Between Physical Health and Autism Spectrum Disorder.
- Shaw, S.C and Carravallah, L and Johnson, M and O'Sullivan, J and Chown, N and Nielson, S and Doherty, M (2024). Barriers to healthcare and a "triple empathy problem" may lead to adverse outcomes for autistic adults: A qualitative study.
- Shaw KA, Williams S, Patrick ME (2022). Prevalence and Early Identification of Autism Spectrum Disorder Among Children Aged 4 and 8 Years - Autism and Developmental Disabilities Monitoring Network, 16 Sites, United States.
- Shawahna, R (2021). Self-rated familiarity with autism spectrum disorders among practicing nurses: a cross-sectional study in the palestinian nursing practice.
- Unknown (2022). Autism-friendly MRI: Improving radiography practice in the UK, a survey of radiographer practitioners.
- Str{"o}mberg, M and Liman, L and Bang, P and Igelstr{"o}m, K (2022). Experiences of Sensory Overload and Communication Barriers by Autistic Adults in Health Care Settings.
- Tong, P and An, I. S (2024). Review of studies applying Bronfenbrenner's bioecological theory in international and intercultural education research [Review]. Frontiers in Psychology, Volume, 14. https://doi.org/10.3389/fpsyg.2023.1233925
- Tromans, S and Chester, V and Kapugama, C and Elliott, A and Robertson, S and Barrett, M (2019). The PAAFID project: exploring the perspectives of autism in adult females among intellectual disability healthcare professionals.
- Urbanowicz, A and Parkin, T and van Dooren, K and Girdler, S and Ciccarelli, M and Lennox, N (2020). The experiences, views, and needs of health professionals who provide care to adults on the autism spectrum.
- Watson-Grace, A and Patel, A and Paradkar, P and Oatney, L and Monroe, T. B and Chipps, E and Tate, J. A and Failla, M. D (2026). Nursing Perspectives on Factors That Influence Provision of Patient-Centered Care for Autistic Patients in a Large Urban Hospital System: A Qualitative Study. Journal of Advanced Nursing. https://doi.org/10.1111/jan.70350
- Zeleke, W. A and Hughes, T. L and Kanyongo, G (2020). Assessing the Effectiveness of Professional Development Training on Autism and Culturally Responsive Practice for Educators and Practitioners in Ethiopia.
- Zerbo, O and Massolo, M. L and Qian, Y and Croen, L. A (2015). A Study of Physician Knowledge and Experience with Autism in Adults in a Large Integrated Healthcare System. Journal of Autism and Developmental Disorders, 45, 4002-4014. https://doi.org/10.1007/s10803-015-2579-2