Abstract
Objective
To examine the average change over time in behaviour, social skills, and quality of life for autistic individuals, and to investigate any potential associations between the outcomes.
Methods
This six-year longitudinal cohort study included 50 participants (aged 7-19 years) with autism spectrum disorder (ASD) from a specialised school. The Aberrant Behaviour Checklist (ABC), Social Responsiveness Scale (SRS) and Pediatric Quality of Life (PedsQL) 4.0 were completed by parents and teachers every 3 months. Mixed-effects models were used to detect significant changes in the mean scores across timepoints, and to examine any longitudinal relationships between the outcomes.
Results
There were statistically significant improvements in the mean teacher-reported ABC (p=0.002), parent-reported SRS (p=0.006), teacher-reported SRS (p=0.003), and PedsQL (p<0.001) over time for all participants, but not for parent-reported ABC (p=0.5). There were significant longitudinal associations between PedsQL and parent-reported ABC (p=0.03), and between PedsQL and SRS (parent: p=0.03; teacher: p=0.001) within an individual.
Conclusions
There were significant improvements in behaviour, social responsiveness, and quality of life in these autistic children and young adults in the specialised school setting. Future studies could explore whether the specialised learning environment, particularly the collaborative and personalised therapeutic care and education programmes, may have led to these improvements in the ASD population.
1. Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that is characterized by deficits in social communication and the presence of restricted, repetitive behaviours or interests. It affects approximately 2.3% of children and 2.2% of adults in the US, and the estimated prevalence has increased over time (Hirota & King, 2023). Often accompanied by other developmental, neurologic, psychiatric and medical conditions, autistic individuals require lifelong support of some kind in many cases (Dang et al., 2017; Levy et al., 2010; Lord et al., 2018). Unfortunately, the necessary coordinated care is not available for many autistic children (Toomey et al., 2013). Moreover, previous studies have rarely reported the inclusion of schools or teachers in outcome measurement of the care approach (Carbone et al., 2010). As such, we initially conducted a school-based pilot study to investigate the feasibility of monitoring outcome measures of autistic children and found that longitudinal data collection from teachers and parents was both feasible and valuable in assisting with individualised education planning and coordinated care for this population (Dang et al., 2017). Therefore, we continued this cohort study over the next six years to observe the change in outcomes among students attending the school. The outcome measures focused on key domains in overall functioning: behaviour, social, and overall quality of life, as measured by the Aberrant Behaviour Checklist (ABC), the Social Responsiveness Scale (SRS) and the Pediatric Quality of Life (PedsQL) 4.0, respectively. Both ABC and SRS are widely used scales for measuring outcomes in ASD research, and can be administered by caregivers, such as parents and teachers (Chun et al., 2021; Kat et al., 2020). We also monitored quality of life, as prior studies found that autistic children have lower quality of life than typically developing children (de Vries & Geurts, 2015; Kuhlthau et al., 2010; van Heijst & Geurts, 2015), and this lower quality of life is strongly associated with more severe autism-related symptoms and traits, as measured by the ABC and SRS (de Vries & Geurts, 2015; Ikeda et al., 2014). Prior longitudinal studies have shown mixed results regarding changes in these outcomes over time, with some showing improvement but then plateauing (Georgiades et al., 2022), some no change (Kuhlthau et al., 2018; Simonoff et al., 2020; Wagner et al., 2019) and others worsening symptoms (Kuhlthau et al., 2010; Rosello et al., 2021). However, there have been no longitudinal studies examining these outcomes in a school environment. Therefore, the primary objective of this cohort study was to investigate the average change over time for parent and teacher-reported aberrant behaviour, social responsiveness, and quality of life for autistic children and young adults at a specialised ASD school. We also wanted to examine whether quality of life was associated with aberrant behaviour and social responsiveness over time in these individuals.
2. Material and methods
The details of this cohort study were described in previous publications (Bent et al., 2020; Dang et al., 2017), but it is briefly described as follows.
2.1. Protocol
The study was approved by the University of California San Francisco Institutional Review Board on April 8, 2014 (approval number 13-11086) prior to performing any study activities. Online questionnaires were completed by parents and special education teachers of the participants approximately every 3 months in an academic school year.
2.2. Participants
Fifty participants (aged between 7-19 years) were recruited from a specialised non-public school (Oak Hill School, San Anselmo, CA) for children and young adults diagnosed with ASD and related neurodevelopmental disorders. The school uses a wide range of evidence-based strategies that centre around relationship building, deeply knowing and understanding the student, and subsequently customising education programmes. The teaching techniques and school environment are detailed in the book, The Oak Hill Method (Bent et al., 2022). They are also summarised in the Appendix. All students diagnosed with ASD (N = 35 at baseline, N = 52 current) were considered as eligible. ASD was defined as being present if the individual had a diagnosis from a medical doctorate psychologist trained to diagnose autism, or if the student was determined by school staff and the study psychiatrist to meet the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition Text-Revision (Diagnostic and Statistical Manual of Mental Disorders, 2013) criteria for ASD. The only exclusion criterion was being unable or unwilling to complete study forms. Participants were enrolled on a rolling basis, leading to staggered entry over the study period and differential follow-up times for the participants (Table 1). Informed consent was obtained from the parents or guardians of all study participants.
Table 1. Data availability and follow-up times for participants (N=50)
| Number of Timepoints | Number of Years in Study | N | % |
|---|---|---|---|
| 4 | 1 | 41 | 82 |
| 7 | 2 | 30 | 60 |
| 10 | 3 | 22 | 44 |
| 12 | 4 | 15 | 30 |
| 15 | 5 | 10 | 20 |
| 18 | 6 | 6 | 12 |
| 20 | 6.5 | 4 | 8 |
2.3. Outcome measures
The core symptoms and co-occuring emotional and behavioural problems of autism were assessed using the Aberrant Behaviour Checklist (ABC) (Aman et al., 1985). It was completed by both parents and teachers, with higher scores indicating more aberrant behaviour. The Social Responsiveness Scale, Second Edition (SRS-2) was used to evaluate social impairment in ASD, (Constantino et al., 2003). It was also reported by both parents and teachers, whereby higher scores denoted greater social impairment. Quality of life was measured by parents only using the Pediatric Quality of Life Inventory 4.0 (PedsQL) (Varni et al., 2001). Covering four domains (physical, emotional, social, and school functioning), higher scores on the PedsQL indicate better quality of life. It has been used in several ASD studies in the past (Ikeda et al., 2013), including longitudinal studies (Kuhlthau et al., 2010).
2.4. Data analytic plan
All statistical analyses were performed using STATA. Descriptive statistics were used to summarise baseline characteristics and variables. Independent t-tests were used to compare the mean scores of the outcomes at baseline with normative data. To evaluate whether there were statistically significant changes in the mean score of ABC, SRS, and PedsQL across the timepoints, repeated measures analysis using linear mixed-effects models was employed. Cohen's d effect sizes were calculated by dividing the change in score (beta coefficient) by the standard deviation of the difference. Parent-reported and teacher-reported ABC and SRS were analysed separately. To examine the association between the change in ABC and SRS and the change in quality of life within an individual over time, linear mixed-effects models were again used. Specifically, we calculated the within-subject association to ensure that the measured change in variables was due to within-individual change rather than between-individual changes. Mixed-effects models also have the advantage of controlling for differences in the number of timepoints of data available between the participants (due to staggered entry into the study); missing data; and attrition, by using the Maximum Likelihood Estimation, which uses all available data to model trajectory. Furthermore, we conducted sensitivity analyses by stratifying the data into length of duration in the study (i.e., participants in the study for one year vs. for two years...etc.) and did not find any qualitative difference in our results after stratification. The models were adjusted for age and sex of the participants. P-values of less than 0.05 were considered statistically significant.
3. Results
3.1. Baseline characteristics
Of the 50 participants in the cohort, 90% were male, and the mean age (and SD) at baseline was 14 ± 3 years, with participants ranging between 7 and 19 years of age (Table 2). The mean ± SD and range of ABC (parent and teacher) score, SRS (parent and teacher) score, and PedsQL score are also shown in Table 1. When compared to previously published data from community samples of autistic children, our study sample had lower mean ABC and SRS scores at baseline, indicating a lower severity in behaviour and social impairment. Our sample had lower PedsQL scores compared to the community sample of typically developing children, indicating better quality of life (Table 3).
Table 2. Sociodemographic characteristics and baseline measures of participants (N=50)
| Measure | N | % | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Age (years) | 47 | - | 14.5 | 3.2 | 7 | 19 |
| Sex | ||||||
| Male | 43 | 89.6 | - | - | - | - |
| Female | 5 | 10.4 | - | - | - | - |
| Aberrant Behaviour Checklist (ABC) | ||||||
| ABC–Parent | 31 | - | 40 | 24.6 | 2 | 128 |
| ABC–Teacher | 40 | - | 46.9 | 23.6 | 7 | 121 |
| Social Responsiveness Scale (SRS) | ||||||
| SRS–Parent | 31 | - | 95 | 25.8 | 36 | 151 |
| SRS–Teacher | 31 | - | 87.1 | 24.2 | 45 | 129 |
| Quality of Life | ||||||
| PedsQL | 29 | - | 47.1 | 16.4 | 18.5 | 82.6 |
Note. N = Sample size; SD = Standard deviation
Table 3. Comparison of baseline mean scores of study sample to established norms
| Measure | Study Sample | Normative Population | t (p) |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Aberrant Behaviour Checklist (ABC) | |||
| ABC–Parent | 40.0 (24.6) | 50.2 (17.8) | 3.1 (0.002)* |
| ABC–Teacher | 46.9 (23.6) | 50.2 (17.8) | 1.2 (0.3) |
| Social Responsiveness Scale (SRS) | |||
| SRS–Parent | 95.0 (25.8) | 117.1 (22.2) | 2.5 (0.01)* |
| SRS–Teacher | 87.1 (24.2) | 117.1 (22.2) | 3.6 (0.0001)* |
| Quality of Life | |||
| PedsQL | 47.1 (16.4) | 80.9 (16.7) | -10.8 (<0.001)* |
Note. Mean scores from the study samples of Kaat et al. (2014), Constantino et al. (2003), and Varni et al. (2001) were used for ABC, SRS, and PedsQL scores respectively, for comparison to the current study. SD = Standard deviation; t = t-statistic *p<0.05
3.2. Change in outcomes over time
On average, there was statistically significant improvement in all outcomes over time. Particularly, teacher-reported ABC (p=0.002), parent-reported SRS (p=0.006), teacher-reported SRS (p=0.003), and quality of life (p<0.001) all showed significant changes, but parent-reported ABC did not (Table 4, Figures 1-3).
Table 4. Change in mean ABC, SRS and PedsQL scores over time, for every survey timepoint.
| Measure | N | β | SE | 95% CI | p |
|---|---|---|---|---|---|
| Aberrant Behaviour Checklist (ABC) | |||||
| ABC–Parent | 47 | -0.12 | 0.2 | -0.5 to 0.3 | 0.5 |
| ABC–Teacher | 48 | -0.52 | 0.2 | -0.9 to -0.2 | 0.002* |
| Social Responsiveness Scale (SRS) | |||||
| SRS–Parent | 43 | -0.7 | 0.3 | -1.2 to -0.2 | 0.006* |
| SRS–Teacher | 46 | -0.72 | 0.2 | -1.2 to -0.2 | 0.003* |
| Quality of Life | |||||
| Pediatric Quality of Life (PedsQL) | 46 | 0.98 | 0.2 | 0.7 to 1.3 | <0.001* |
Note. N = Sample size; β = Beta coefficient; SE = Standard error; 95% CI = 95% confidence intervals. *p<0.05
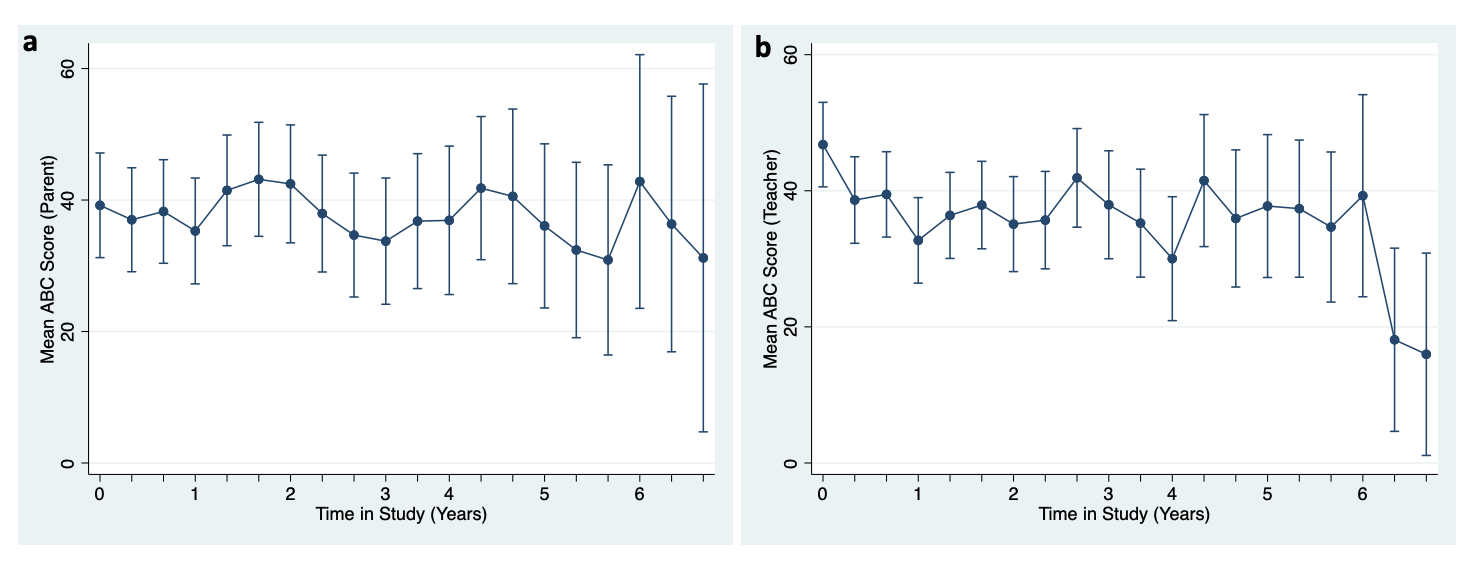
Compared to baseline, teacher-reported ABC decreased by 8.84 points (p=0.03) and teacher-reported SRS decreased by 24.2 points (p=0.01) after three years, corresponding to a small effect size (Table 4). Similarly, quality of life scores increased by 13.2 points (p<0.001) after 3 years in the study compared to baseline, indicating a moderate effect (Table 5). Parent-reported ABC and SRS scores also decreased after three years, but these changes were not statistically significant.
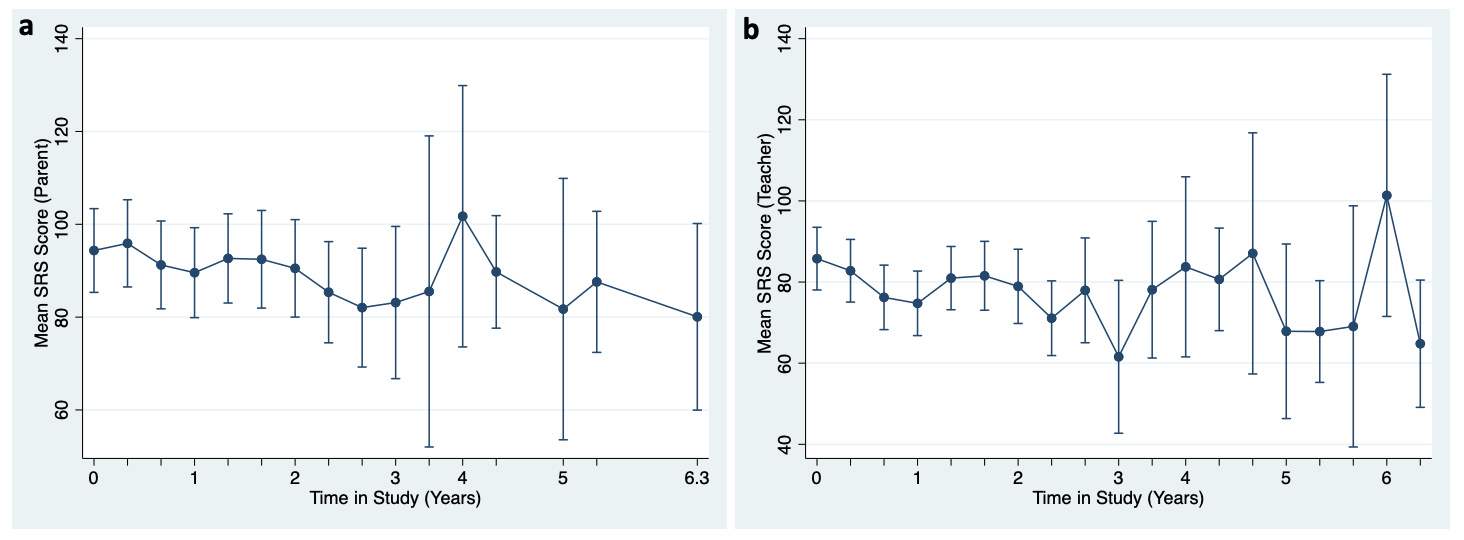
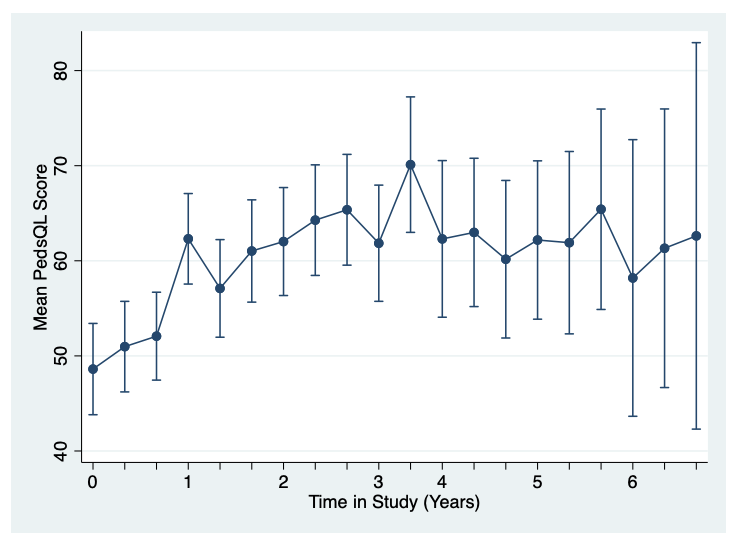
Table 5. Change in mean ABC, SRS and PedsQL scores after three years in the study compared to baseline
| Measure | N | β | SE | 95% CI | Effect size | p |
|---|---|---|---|---|---|---|
| Aberrant Behaviour Checklist (ABC) | ||||||
| ABC–Parent | 47 | -5.45 | 4.4 | -14 to 3.1 | -0.18 | 0.2 |
| ABC–Teacher | 48 | -8.84 | 4.1 | -16.8 to -0.8 | -0.31 | 0.03* |
| Social Responsiveness Scale (SRS) | ||||||
| SRS–Parent | 43 | -11.2 | 7.9 | -26.6 to 4.2 | -0.22 | 0.15 |
| SRS–Teacher | 46 | -24.2 | 9.6 | -43 to -5.4 | -0.37 | 0.01* |
| Quality of Life | ||||||
| Pediatric Quality of Life (PedsQL) | 46 | 13.2 | 3.3 | 6.7 to 19.8 | 0.58 | <0.001* |
Note. N = Sample size; β = Beta coefficient; SE = Standard error; 95% CI = 95% confidence intervals. *p<0.05
3.3. Longitudinal associations between outcomes
Overall, there were statistically significant associations between change in ABC and SRS scores and change in quality of life over time. Namely, we found that within an individual, improvements in parent-reported ABC and SRS (both parent- and teacher-reported) were associated with improvements in PedsQL over time, both in unadjusted analyses and after adjusting for age and sex (Table 6). Teacher-reported ABC did not show any such association.
Table 6. Crude and adjusted associations between ABC and PedsQL, and between SRS and PedsQL over time within an individual
| Measure | N | β | SE | 95% CI | p | |
|---|---|---|---|---|---|---|
| Quality of Life | ||||||
| Aberrant Behaviour Checklist–Parent | Unadjusted | 46 | -0.13 | 0.06 | -0.3 to -0.1 | 0.006* |
| Adjusteda | 44 | -0.12 | 0.06 | -0.2 to -0.01 | 0.03* | |
| Aberrant Behaviour Checklist–Teacher | Unadjusted | 44 | -0.04 | 0.06 | -0.2 to 0.1 | 0.4 |
| Adjusteda | 42 | -0.02 | 0.05 | -0.1 to 0.1 | 0.7 | |
| Social Responsiveness Scale–Parent | Unadjusted | 42 | -0.11 | 0.05 | -0.2 to -0.01 | 0.03* |
| Adjusteda | 41 | -0.11 | 0.05 | -0.2 to -0.01 | 0.03* | |
| Social Responsiveness Scale–Teacher | Unadjusted | 44 | -0.16 | 0.05 | -0.3 to -0.06 | 0.001* |
| Adjusteda | 43 | -0.16 | 0.05 | -0.3 to -0.07 | 0.001* |
Note. N = Sample size; β = Beta coefficient; SE = Standard error; 95% CI = 95% confidence intervals.aModels adjusted for age and sex of the participants *p<0.05
4. Discussion
In this six-year long cohort study of students in a specialised ASD school, we found a significant improvement in aberrant behaviour, social responsiveness, and quality of life (except parent-reported aberrant behaviour) over time, as well as significant longitudinal associations between aberrant behaviour and social responsiveness with quality of life. Although causality could not be determined in this study, there may be a possibility that the specialised education environment (see Appendix) in this school may be fostering a positive change, which would be a topic for future research. At baseline, our participants had lower quality of life scores compared to the normative sample of typically developing children (Varni et al., 2001), aligning with past literature that has associated autism with a lower quality of life (de Vries & Geurts, 2015; Ikeda et al., 2014; Kuhlthau et al., 2010; van Heijst & Geurts, 2015). Interestingly, our participants had better aberrant behaviour and social responsiveness scores at baseline compared to the normative samples of other autistic children (Constantino et al., 2003; Kaat et al., 2014). That being said, due to differences in sampling frames, era, and severity, direct comparisons of our results with the normative samples should be interpreted with caution. These normative scores were included as a reference point when viewing the baseline scores in this study. Furthermore, all references to baseline measurements are simply the first measurements taken after enrolling in the cohort study, which may not be considered entry-level functioning for participants who had been in the school prior to enrolment in the study. After three years in the study, there was a small but significant improvement in teacher-reported aberrant behaviour and social responsiveness and a moderate improvement in quality of life, compared to baseline. These modest improvements are important for long-term functioning and may be argued to be robust. It is important to note that this was a heterogenous population, where not every participant showed the same trajectory when it came to the outcomes; some showed improvement across all outcomes, some had improvement in one but not the others, whereas some did not have any significant changes in their scores, or even slight worsening. For instance, one participant, a 15-year-old male who was in the study for three years, showed remarkable improvement across all outcomes. On the other hand, another participant, a 16-year-old male who was in the study for 6 years, showed a trajectory where initially there was strong improvement in all outcomes (about three years into the study) but then regressed to worse scores in the second half of their time there, with an overall slight improvement in some outcomes but no change in the others. Despite the varying findings at an individual level, there was significant improvement on average at the population level for all outcomes. Our results are in contrast with the few longitudinal studies examining these outcomes, which have mostly shown that aberrant behaviour, social responsiveness, and quality of life remain unchanged or worsen over time. For instance, a cohort study by Wagner et al. (2022) did not find any changes to both parent and teacher-reported measures of SRS from preschool to young adulthood. Similarly, another study following autistic individuals showed no change in SRS over time and also found mainstream school attendance to be a predictor of better outcomes (Simonoff et al., 2020). Considering that the school from which our study sample was taken was not a mainstream school, our findings are especially significant. Another study found that regardless of the level of ASD symptom severity, at the 5-year follow-up, autistic participants had more difficulties in peer relationships and low social competence in school settings compared to typically developing participants (Rosello et al., 2021). Even studies showing improvement in autism symptoms have some caveats, such as one that found 73% of the sample of autistic children had an ``improving then plateauing'' trajectory (Georgiades et al., 2022). As such, the continuous improvement of outcomes seen in our findings is noteworthy. In regard to quality of life, previous studies have found no change (Kuhlthau et al., 2010) or a decrease over time (Kuhlthau et al., 2018) in autistic individuals. Therefore, our results showing an improvement in quality of life is of particular significance. Furthermore, this improvement in quality of life being significantly associated to the improvement in ABC and SRS scores confirm the results of previous cross-sectional studies, where having higher quality of life was associated with having fewer impairments in social skills and behaviour (de Vries & Geurts, 2015; Ikeda et al., 2014; Kuhlthau et al., 2010), and demonstrate that these associations remain over time as well. Many of the previous studies had pointed out that behavioural interventions for autistic children may also improve quality of life (Cottenceau et al., 2012; Dijkhuis et al., 2017; Kuhlthau et al., 2010). In the current study, it is possible that individuals who enrol at this specialised school for ASD may have experienced improvements in behaviour and social responsiveness, which may have led to improvement in their quality of life as well, although causality cannot be determined at this point. An interesting finding in the study was the improvement in teacher-reported aberrant behaviour in contrast to parent-reported aberrant behaviour, suggesting that aberrant behaviour may have manifested differently depending on the environment, i.e., aberrant behaviour in the home environment (measured by parents) may be different from that in the classroom (measured by teachers). Discrepancies in informants' (parents, teachers, children) ratings of child and adolescent psychopathology have often been reported in the literature (De Los Reyes, 2019). These discrepancies, which have been shown to be stable over time, reveal meaningful differences that can better help us understand psychosocial functioning (De Los Reyes, 2019; De Los Reyes et al., 2019). For instance, it has been observed that executive function challenges experienced by autistic children are not identical across school and home settings and that support may differ in each setting (Tschida & Yerys, 2022). Perhaps a similar phenomenon is the case for aberrant behaviour as well. Even if the behaviours were similar in both contexts, parents and teachers may have rated them differently as teachers may be able to compare the participant to the many other autistic students in the class whereas parents rarely have as many children to similarly ``standardise'' their rating of aberrant behaviour in ASD. Further research is required to delineate how aberrant behaviour in ASD may be manifested in different environments and contexts. There is also a possibility of the difference in rater-based findings being influenced by contextual bias on the teachers' end. Nevertheless, these results demonstrate the value of including teacher reports and adding them as a care point in care coordination. In future studies, in addition to parents and teachers' input, peers could be yet another perspective of relevance, especially since peer relationships play a role in social behaviours and quality of life, where neurotypical peers could be objective raters of participants' social interactions in the school setting. It is also significant to note that the ABC includes a suite of behaviours coded as ``stereotypic,'' and the SRS includes a suite of behaviours coded as ``restrictive interests - repetitive behaviour.'' The Oak Hill School staff is trained to view many of those behaviours not as aberrant or anti-social but rather as potentially constructive, generative attempts on the part of the student to achieve sensory or emotional self-regulation, or to communicate wants and needs (Bent et al., 2022). Thus, it may be that those suites of behaviours were not observed to decrease as much as other domains of behaviours in both teacher and parent reporting on the ABC and the SRS. This study has several limitations that should be acknowledged. Firstly, due to the observational nature of the research and the possibility of unmeasured confounding, the improvement in outcomes over time cannot be attributed to the school itself. Therefore, we cannot claim any causality in these findings. Similarly, the associations of ABC and SRS with quality of life are also not causal in nature. In addition, we did not have a control group, further limiting our ability to isolate the effect of the school environment from other confounding factors. Nevertheless, we attempted to control for confounders by adjusting for age and sex of the participants using multivariate models. We also did not have any data on pharmacological or psychosocial intervention, intensity of services, IQ, adaptive functioning, or co-occuring psychiatric conditions for the participants, all of which may have influenced our findings. Particularly, medications targeting irritability could have affected ABC scores. Another constraint is the small sample size, which may have led to a lack of precision in estimates of the beneficial effects. Finally, due to the staggered entry design as well as participants graduating from the school, only a small proportion of the participants were in the study for the full six years, with the majority being in the study for three years. However, this imbalance was accounted for in the analysis with the mixed-effects model to measure change, since it is better at dealing with missing data in comparison to other repeated measures analyses.
5. Conclusions
We believe this study presents important findings regarding longitudinal changes in aberrant behaviour, social responsiveness, and quality of life in a specialised school environment and is noteworthy as one of the few to include teachers and schools in care coordination. To our knowledge, this is the first such cohort study to show significant improvement in these domains among autistic individuals in a school environment. Future research could explore whether the specialised learning environment, particularly the collaborative and personalised therapeutic care and education programmes, may have led to these improvements in this ASD population. Future studies could also determine factors associated with greatest and least improvement, with hope of matching focused treatment. We would like to thank all the parents, teachers and staff members who participated in this study. This work was supported by the JS Foundation. JS Foundation had no involvement in the study design, the collection, analysis and interpretation of data, the writing of the report, or in the decision to submit the article for publication. Bushra Hossain and Michael G. McDonald report current employment at Oak Hill School. At the time of the study and initial preparation for publication, Bushra Hossain was affiliated solely with University of California San Francisco. All other authors declare that they have no conflicts of interest.
References
- Aman, M. G and Singh, N. N and Stewart, A. W and Field, C. J (1985). The aberrant behaviour checklist: A behaviour rating scale for the assessment of treatment effects. American Journal of Mental Deficiency, 89.
- Bastiaansen, D and Koot, H. M and Bongers, I. L and Varni, J. W and Verhulst, F. C (2004). Measuring quality of life in children referred for psychiatric problems: Psychometric properties of the PedsQL 4. Journal, 0. https://doi.org/10.1023/B:QURE.0000018483.01526.ab
- Bent, S and McDonald, M. G and Hendren, R. L (2022). The Oak Hill Method: Connecting to Students with Autism.
- Bent, S and Wahlberg, J and Chen, Y and Widjaja, F and McDonald, M. G and Hendren, R. L (2020). Quality of Life Among School-Age Children With Autism: The Oak Hill School Outcomes Study. Seminars in Pediatric Neurology, 34. https://doi.org/10.1016/j.spen.2020.100808
- Carbone, P. S and Behl, D. D and Azor, V and Murphy, N. A (2010). The medical home for children with autism spectrum disorders: Parent and pediatrician perspectives. Journal of Autism and Developmental Disorders, 40. https://doi.org/10.1007/s10803-009-0874-5
- Channell, M. M (2020). The Social Responsiveness Scale (SRS-2) in school-age children with Down syndrome at low risk for autism spectrum disorder. Autism & Developmental Language Impairments, 5. https://doi.org/10.1177/2396941520962406
- Chun, J and Bong, G and Han, J. H and Oh, M and Yoo, H. J (2021). Validation of Social Responsiveness Scale for Korean Preschool Children With Autism. Psychiatry Investigation, 18. https://doi.org/10.30773/pi.2021.0182
- Constantino, J. N and Davis, S. A and Todd, R. D and Schindler, M. K and Gross, M. M and Brophy, S. L and Metzger, L. M and Shoushtari, C. S and Splinter, R and Reich, W (2003). Validation of a brief quantitative measure of autistic traits: Comparison of the social responsiveness scale with the autism diagnostic interview-revised. Journal of Autism and Developmental Disorders, 33. https://doi.org/10.1023/a:1025014929212
- Cottenceau, H and Roux, S and Blanc, R and Lenoir, P and Bonnet-Brilhault, F and Barthélémy, C (2012). Quality of life of adolescents with autism spectrum disorders: Comparison to adolescents with diabetes. European Child & Adolescent Psychiatry, 21. https://doi.org/10.1007/s00787-012-0263-z
- Dang, K and Bent, S and Lawton, B and Warren, T and Widjaja, F and McDonald, M. G and Breard, M and O'Keefe, W and Hendren, R. L (2017). Integrating Autism Care through a School-Based Intervention Model: A Pilot Study. Journal of Clinical Medicine, 6. https://doi.org/10.3390/jcm6100097
- De Los Reyes, A (2019). Introduction to the special section: More than measurement error: Discovering meaning behind informant discrepancies in clinical assessments of children and adolescents.
- De Los Reyes, A and Cook, C. R and Gresham, F. M and Makol, B. A and Wang, M (2019). Informant discrepancies in ssessments of psychosocial functioning in school-based services and research: Review and directions for future research. J Sch Psychol, 74, 74-79. https://doi.org/10.1016/j.jsp.2019.05.005.
- de Vries, M and Geurts, H (2015). Influence of Autism Traits and Executive Functioning on Quality of Life in Children with an Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 45. https://doi.org/10.1007/s10803-015-2438-1
- Dijkhuis, R. R and Ziermans, T. B and Van Rijn, S and Staal, W. G and Swaab, H (2017). Self-regulation and quality of life in high-functioning young adults with autism. Autism, 21. https://doi.org/10.1177/1362361316655525
- Georgiades, S and Tait, P. A and McNicholas, P. D and Duku, E and Zwaigenbaum, L and Smith, I. M and Bennett, T and Elsabbagh, M and Kerns, C. M and Mirenda, P and Ungar, W. J and Vaillancourt, T and Volden, J and Waddell, C and Zaidman-Zait, A and Gentles, S and Szatmari, P (2022). Trajectories of Symptom Severity in Children with Autism: Variability and Turning Points through the Transition to School. Journal of Autism and Developmental Disorders, 52. https://doi.org/10.1007/s10803-021-04949-2
- Hirota, T and King, B. H (2023). Autism Spectrum Disorder: A Review. JAMA, 329. https://doi.org/10.1001/jama.2022.23661
- Ikeda, E and Hinckson, E and Krägeloh, C (2014). Assessment of quality of life in children and youth with autism spectrum disorder: A critical review. Quality of Life Research, 23. https://doi.org/10.1007/s11136-013-0591-6
- Kaat, A. J and Lecavalier, L and Aman, M. G (2014). Validity of the aberrant behaviour checklist in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44. https://doi.org/10.1007/s10803-013-1970-0
- Kat, S and Xu, L and Guo, Y and Ma, J and Ma, Z and Tang, X and Yang, Y and Wang, H and Li, X and Liu, J (2020). Reliability and Validity of the Simplified Chinese Version of the Aberrant Behaviour Checklist in Chinese Autism Population. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.545445
- Kuhlthau, K. A and McDonnell, E and Coury, D. L and Payakachat, N and Macklin, E (2018). Associations of quality of life with health-related characteristics among children with autism. Autism: The International Journal of Research and Practice, 22. https://doi.org/10.1177/1362361317704420
- Kuhlthau, K and Orlich, F and Hall, T. A and Sikora, D and Kovacs, E. A and Delahaye, J and Clemons, T. E (2010). Health-Related Quality of Life in children with autism spectrum disorders: Results from the autism treatment network. Journal of Autism and Developmental Disorders, 40. https://doi.org/10.1007/s10803-009-0921-2
- Levy, S. E and Giarelli, E and Lee, L.-C and Schieve, L. A and Kirby, R. S and Cunniff, C and Nicholas, J and Reaven, J and Rice, C. E (2010). Autism spectrum disorder and co-occurring developmental, psychiatric, and medical conditions among children in multiple populations of the United States. Journal of Developmental and Behavioural Pediatrics: JDBP, 31. https://doi.org/10.1097/DBP.0b013e3181d5d03b
- Lord, C and Elsabbagh, M and Baird, G and Veenstra-Vanderweele, J (2018). Autism spectrum disorder. Lancet (London, England), 392. https://doi.org/10.1016/S0140-6736(18)31129-2
- Rosello, R and Berenguer, C and Martinez-Raga, J and Miranda, A and Cortese, S (2021). Subgroups of Children with Autism Spectrum Disorder without Intellectual Disability: A Longitudinal Examination of Executive and Socio-Adaptive Behaviours in Adolescence. Journal of Clinical Medicine, 10. https://doi.org/10.3390/jcm10102220
- Schmidt, J. D and Huete, J. M and Fodstad, J. C and Chin, M. D and Kurtz, P. F (2013). An Evaluation of the Aberrant Behaviour Checklist for Children Under Age 5. Research in Developmental Disabilities, 34. https://doi.org/10.1016/j.ridd.2013.01.002
- Simonoff, E and Kent, R and Stringer, D and Lord, C and Briskman, J and Lukito, S and Pickles, A and Charman, T and Baird, G (2020). Trajectories in Symptoms of Autism and Cognitive Ability in Autism From Childhood to Adult Life: Findings From a Longitudinal Epidemiological Cohort. Journal of the American Academy of Child and Adolescent Psychiatry, 59. https://doi.org/10.1016/j.jaac.2019.11.020
- Tschida, J. E and Yerys, B. E (2022). Real-world executive functioning for autistic children in school and home settings. Autism: The International Journal of Research and Practice, 26. https://doi.org/10.1177/13623613211041189
- Toomey, S. L and Chien, A. T and Elliott, M. N and Ratner, J and Schuster, M. A (2013). Disparities in unmet need for care coordination: The national survey of children's health. Pediatrics, 131. https://doi.org/10.1542/peds.2012-1535
- van Heijst, B. F. C and Geurts, H. M (2015). Quality of life in autism across the lifespan: A meta-analysis. Autism: The International Journal of Research and Practice, 19. https://doi.org/10.1177/1362361313517053
- Varni, J. W and Seid, M and Kurtin, P. S (2001). PedsQL 4. Journal, 0. https://doi.org/10.1097/00005650-200108000-00006
- Wagner, R. E and Zhang, Y and Gray, T and Abbacchi, A and Cormier, D and Todorov, A and Constantino, J. N (2019). Autism‐Related Variation in Reciprocal Social Behaviour: A Longitudinal Study. Child Development, 90. https://doi.org/10.1111/cdev.13170