Abstract
Aim
This study aimed to compare the effectiveness of a hospital-based sports rehabilitation program (SRP) versus a home-based exercise program (HEP) on motor function, participation-related, and therapy engagement outcomes in children with developmental disabilities and to evaluate feasibility and safety.
Methods
This exploratory randomized pilot study allocated 16 children to SRP or HEP (1:1) using block randomization stratified by Gross Motor Function Classification System (GMFCS) level. Both interventions were delivered for 8 weeks. Outcomes included Gross Motor Function Measure (GMFM), Pediatric Balance Scale (PBS), Canadian Occupational Performance Measure (COPM-Performance/Satisfaction), Pediatric Volitional Questionnaire (PVQ), and Goal Attainment Scaling (GAS; T-score). A 2×2 mixed ANOVA (group × time) was used for most outcomes, and an independent t-test was used for GAS T-scores.
Results
Both groups showed significant improvements over time in GMFM and PBS (p < 0.001). Group-by-time interactions favored SRP for COPM-Performance (p = 0.038), COPM-Satisfaction (p = 0.025), and PVQ (p = 0.038). The GAS T-scores did not differ between the groups (p = 0.645). Feasibility criteria were met (≥75% adherence, fidelity, and exercise dose).
Conclusion
Both interventions were feasible and safe over 8 weeks. The SRP was associated with relatively more favorable participation-related outcomes. Future adequately powered trials with a longer follow-up period are warranted to confirm these findings.
1. Introduction
Children with developmental disabilities, including cerebral palsy, autism spectrum disorder, and genetic or chromosomal disorders, often show combined cognitive, motor, and social limitations that restrict daily function and engagement in rehabilitation (Bhat, 2021; Imms et al., 2017). Reduced engagement can disrupt treatment continuity and limit long-term effectiveness, making gross motor function improvement alongside active participation a key clinical goal (Imms et al., 2017; Novak et al., 2013; Tatla et al., 2013). Sports-based rehabilitation has been increasingly adopted in pediatric settings and may improve coordination, balance, and mobility (Healy et al., 2018; Ruggeri et al., 2020). Structured, repetitive practice may facilitate functional gains through skill acquisition (Bishop & Pangelinan, 2018), and motivation and peer interaction can be enhanced by group-based activities. However, the time burden, access limitations, and variable caregiver availability often limit clinic-based delivery, which may hinder sustained participation (Ballantyne et al., 2019; Xie et al., 2024). Caregiver-led home-based exercise programs offer an alternative or complementary model by embedding practice in daily routines and positioning caregivers as co-interventionists (Guralnick, 2011; King et al., 2004). Caregiver involvement and ongoing support have been associated with improvements in motor performance and therapy-related engagement and may facilitate adherence and goal attainment in home-based rehabilitation (Lillo-Navarro et al., 2019). Despite the positive findings, direct comparisons using standardised outcomes remain limited. Therefore, this exploratory pilot study aimed to assess feasibility and provide a preliminary estimation of potential intervention effects. Specifically, we compared an 8-week hospital-based SRP with a caregiver-led HEP in ambulatory children with developmental disabilities classified as GMFCS levels I-III, evaluating activity-level outcomes (GMFM and PBS), participation-level outcomes and therapy engagement (COPM and PVQ), and safety.
2. Methods
2.1. Ethics
This study was approved by the Institutional Review Board of Yonsei University Mirae Campus (Approval No. 1041849-202508-BM-171-03), and participant recruitment began after approval. Written informed consent was obtained from the legal guardians, and assent was obtained from the children when appropriate. Data were de-identified using study codes and managed according to institutional regulations. This study was conducted in accordance with the principles of the Declaration of Helsinki.
2.2. Participants
Participants were children and adolescents (8-15 years) with developmental disabilities (e.g., autism spectrum disorder, cerebral palsy, and chromosomal disorders). Eligible participants were those classified as standard GMFCS levels I-III (individuals with levels IV and V were excluded). These criteria targeted a population capable of walking independently or with minimal assistance, following multi-step instructions, and safely participating in ~30-minute exercise sessions. Furthermore, participants must have received rehabilitation therapy within the past 6 months and have a caregiver available to support home participation. The exclusion criteria were as follows: medical instability limiting safe exercise, recent surgery (<6 months) or botulinum toxin injection (<4 months), moderate-to-severe sensory impairment, severe behavioural/emotional problems affecting safety, concurrent participation in similar programs, or caregiver inability to participate. The target sample comprised 16 participants (8 per group). As this was a low-risk QI exploratory pilot study, the sample size was determined pragmatically based on feasible recruitment and the clinical capacity to deliver safe small-group rehabilitation sessions, rather than through a formal power calculation. Because the study was not designed or powered for definitive hypothesis testing, this pragmatic approach was consistent with its dual aims: to assess feasibility (recruitment/retention, implementation fidelity, and safety) and to generate preliminary estimates of intervention effects (Leon et al., 2011). Accordingly, this sample should be regarded as appropriate for pilot feasibility purposes, but not for drawing confirmatory conclusions regarding efficacy. The GMFCS level was recorded to describe the functional status at baseline. Although GMFCS was developed for cerebral palsy, it was used conservatively as a functional descriptor across heterogeneous diagnoses, and interpretations were made accordingly (Palisano et al., 1997).
2.3. Study Design
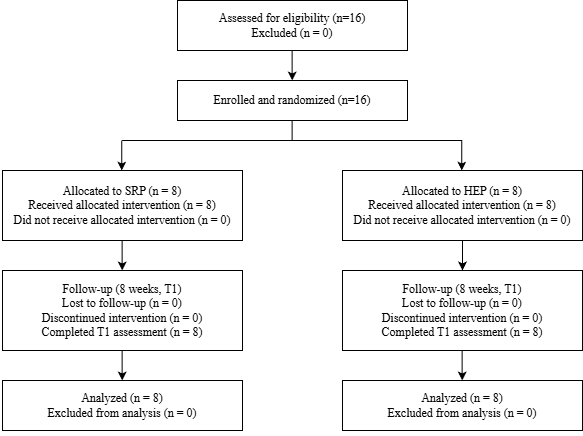
This was an 8-week, exploratory randomised pilot study (parallel-group) conducted in a single tertiary hospital rehabilitation setting in Seoul, South Korea. Participant recruitment occurred in 2025. Participants were individually randomised (1:1) to a hospital-based SRP or a HEP. Randomisation was stratified according to the GMFCS level (I-III) and implemented using a prespecified permuted-block sequence. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared and administered by an independent third party not involved in recruitment, intervention delivery, or outcome assessment. The blinding of participants and intervention therapists was not feasible. Outcome assessments were conducted by assessors blinded to group allocation. Assessments were performed at baseline (T0) and 8 weeks after the intervention (T1) using standardised procedures (scripted instructions, assessor training, and predefined scoring criteria). New concurrent therapies during the intervention period were discouraged to reduce confounding from co-interventions. Usual care was requested to remain stable when possible, and any changes (type, frequency, and duration) were recorded using a standardised log. Figure 1 shows the flow of the participants.
2.4. Outcome Measures
Outcomes were prespecified as primary (motor function and balance), secondary (participation and engagement), and exploratory (goal attainment) measures based on clinical relevance. Primary and secondary outcomes were assessed at T0 and T1, whereas the exploratory GAS T-scores were derived from goal attainment ratings only at T1, reflecting the inherent design of the tool. COPM and GAS were administered using researcher-defined standardised common goals aligned with the intervention tasks and instrument requirements rather than individualised goals to enable between-group comparison using common sport-related functional task demands (Kiresuk & Sherman, 1968; Law et al., 1990). The same prespecified goal set and standardised rating anchors (detailed in Supplementary File S1) were applied in both groups according to the study protocol. Primary outcomes: GMFM (0-100%) and PBS (0-56) were assessed. GMFM summarised gross motor performance as a percentage score based on standardised item performance (Russell et al., 1989). PBS quantified functional balance performance across sitting, standing, and weight-shift tasks with a total score ranging from 0 to 56 (Franjoine et al., 2003). Secondary outcomes: COPM-Performance and COPM-Satisfaction (1-10) captured caregiver ratings for the prespecified common goal tasks (Law et al., 1990). The PVQ (15-60) was used to assess the observed volition and engagement during the usual-care therapy sessions using standardised anchors. The usual-care therapist, who was blinded to group allocation, rated the PVQ, and the rater received prespecified training on anchor use and scoring procedures (Andersen et al., 2005). Exploratory outcome: GAS T-scores at T1 were derived from goal attainment ratings for the standardised common goals using a 5-point scale from -2 to +2 and converted to T-scores based on the original GAS framework (Kiresuk & Sherman, 1968). The findings of the GAS were interpreted in the context of evidence from pediatric rehabilitation (Steenbeek et al., 2007).
2.5. Intervention Protocol
SRP: Participants in the SRP group attended supervised sessions delivered by a physical therapist who also held a certified sports coaching qualification, in a designated hospital space, twice weekly for 45 minutes over 8 weeks (16 sessions). Each session included a warm-up, task-oriented core activities, and a cool-down. The core activities included static/dynamic balance, coordination/agility, functional mobility, and small-group game-based sports skills. Motor learning principles were followed for function-based pediatric interventions (Levac et al., 2009). The exercise intensity was individualised to an OMNI Rating of Perceived Exertion (OMNI-RPE) of 5-7 (0-10 scale) (Utter et al., 2002). The task difficulty was progressed using a standardised performance-based rule. The next difficulty level was introduced when the target quality of performance was achieved on the same task in two consecutive opportunities under standardised conditions consistent with the principles of progressive overload (ACSM, 2009). HEP: The HEP group completed caregiver-led home sessions three times weekly for approximately 30 minutes over 8 weeks (24 sessions). Before initiation, caregivers received standardised instruction (~30 minutes) on task execution, safety, and recording procedures. During the program, weekly telephone coaching (10-15 minutes) was provided to monitor adherence, provide feedback on performance errors, and adjust task difficulty when needed. The intervention content and intensity targets were aligned with the SRP (OMNI-RPE 5-7) (Utter et al., 2002), and the same progression rule was applied (ACSM, 2009). Implementation fidelity and safety monitoring: Implementation fidelity and feasibility were assessed using prespecified adherence metrics, including session completion (SRP: attendance-based; HEP: completion-based), coaching participation (HEP), weekly exercise time (min/week), and total exercise time over 8 weeks (min). Feasibility success was defined a priori as achieving a ≥75% threshold for each metric. This pragmatic clinical benchmark accommodates the population's logistical challenges and aligns with the methodological guidelines for pilot progression criteria (Thabane et al., 2010). Safety was monitored by documenting adverse events, defined as any untoward medical occurrence during participation requiring task modification, temporary suspension, or medical evaluation (e.g., falls, musculoskeletal injury, marked pain exacerbation, dizziness, or cardiopulmonary symptoms). When an adverse event occurred, the intervention was modified or discontinued as appropriate, and events were documented and reported according to institutional procedures.
2.6. Statistical Analysis
All analyses were performed using IBM SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA). Categorical variables are presented as n (%), and continuous variables as mean ± SD or median (IQR), as appropriate. The normality and homogeneity of variance were assessed using the Shapiro-Wilk and Levene's tests, respectively. Since all primary outcome variables met these assumptions, parametric mixed ANOVAs were employed for the repeated-measures analyses, obviating the need for nonparametric alternatives. Baseline characteristics were compared using the independent-samples t-test or Mann-Whitney U test for continuous variables and Fisher's exact test for categorical variables. For outcomes measured at T0 and T1, a two-way mixed ANOVA was conducted with group (SRP vs. HEP) and time (T0 vs. T1) as the between-subject and within-subject factors, respectively. The effect sizes for the ANOVA results were reported as partial η². The GAS T-scores measured at T1 were compared between groups using an independent-samples t-test, with Cohen's d reported as the effect size. The analyses followed the intention-to-treat principle. There were no missing outcome data; therefore, no imputation was required. All tests were two-sided with an alpha level of 0.05.
3. Results
At baseline, no between-group differences in demographic or clinical characteristics were observed (all p > 0.05), supporting baseline comparability (Table 1).
Table 1. Baseline Characteristics of the Participants
| Variables | SRP (n=8) | HEP (n=8) | p-value |
|---|---|---|---|
| Age (years) | 9.5 (8.0–11.8) | 10.0 (8.0–12.8) | 0.745 |
| Weight (kg) | 29.4 (25.3–38.9) | 33.9 (27.6–39.1) | 0.563 |
| Height (cm) | 125.0 (117.2–137.0) | 123.1 (115.9–132.3) | 0.713 |
| Sex (M/F) | 6/2 | 7/1 | 1.000 |
| GMFCS (I/II/III) | 5/2/1 | 4/2/2 | 0.801 |
Note. Values are median (IQR) or n. SRP = sports rehabilitation program; HEP = home-based exercise program; GMFCS = Gross Motor Function Classification System.
For primary outcomes, GMFM and PBS improved from T0 to T1, as shown by significant main effects of time (GMFM: p < 0.001, partial η² = 0.584; PBS: p < 0.001, partial η² = 0.658) (Table 2). No significant main effects of group were observed (GMFM: p = 0.347; PBS: p = 0.711), and group × time interactions were not significant (GMFM: p = 0.492; PBS: p = 0.149), indicating similar pre-post changes across SRP and HEP (Table 2).
Table 2. Primary Outcomes (GMFM and PBS)
| Two-way mixed ANOVA | ||||||
|---|---|---|---|---|---|---|
| Outcome | Group | Pre Mean ± SD | Post Mean ± SD | Time p (η²) | Group p (η²) | Interaction p (η²) |
| GMFM | SRP | 88.2 ± 5.7 | 89.8 ± 5.3 | < 0.001 (0.584) | 0.347 (0.063) | 0.492 (0.034) |
| HEP | 85.1 ± 8.1 | 86.2 ± 8.0 | ||||
| PBS | SRP | 42.5 ± 4.8 | 43.9 ± 4.7 | < 0.001 (0.658) | 0.711 (0.010) | 0.149 (0.143) |
| HEP | 41.5 ± 8.5 | 42.3 ± 8.8 | ||||
Note. Values are mean ± SD. GMFM = Gross Motor Function Measure; PBS = Pediatric Balance Scale; SRP = sports rehabilitation program; HEP = home-based exercise program; η² = partial eta squared.
For secondary outcomes, COPM-Performance and COPM-Satisfaction increased over time (COPM-P: p < 0.001, partial η² = 0.729; COPM-S: p < 0.001, partial η² = 0.775) without significant main effects of group (COPM-P: p = 0.329; COPM-S: p = 0.303) (Table 3). Significant group × time interactions were observed for both COPM measures (COPM-P: p = 0.038, partial η² = 0.272; COPM-S: p = 0.025, partial η² = 0.311), indicating greater improvement in SRP compared with HEP over time (Table 3). The PVQ showed significant main effects of time (p < 0.001, partial η² = 0.838) and group (p = 0.035, partial η² = 0.281), as well as a significant group × time interaction (p = 0.038, partial η² = 0.272), suggesting greater change over time in SRP, with higher overall scores compared with HEP (Table 3). For the exploratory outcome, GAS T-scores at T1 did not differ between groups (t(14) = 0.471, p = 0.645), with a small effect size (Cohen's d = 0.236; 95% CI [-0.752, 1.215]) (Table 3).
Table 3. Secondary Outcomes (COPM-P, COPM-S, PVQ, and GAS)
| Two-way mixed ANOVA | ||||||
|---|---|---|---|---|---|---|
| Outcome | Group | Pre Mean ± SD | Post Mean ± SD | Time p (η²) | Group p (η²) | Interaction p (η²) |
| COPM - Performance | SRP | 5.6 ± 1.2 | 7.4 ± 1.5 | < 0.001 (0.729) | 0.329 (0.068) | 0.038 (0.272) |
| HEP | 5.4 ± 1.6 | 6.2 ± 1.5 | ||||
| COPM - Satisfaction | SRP | 5.7 ± 1.2 | 7.7 ± 1.2 | < 0.001 (0.775) | 0.303 (0.076) | 0.025 (0.311) |
| HEP | 5.6 ± 1.3 | 6.5 ± 1.4 | ||||
| PVQ | SRP | 37.9 ± 6.0 | 50.9 ± 2.9 | < 0.001 (0.838) | 0.035 (0.281) | 0.038 (0.272) |
| HEP | 33.3 ± 8.5 | 40.8 ± 8.2 | ||||
| Independent t-test | ||||||
| Outcome | Group | Mean ± SD | t(df) | p-value | Cohen's d | 95% CI |
| GAS T-score | SRP | 65.4 ± 17.7 | t (14) = 0.471 | 0.645 | 0.236 | [-0.752, 1.215] |
| HEP | 61.4 ± 16.3 | |||||
Note. Values are mean ± SD. SRP = sports rehabilitation program; HEP = home-based exercise program; COPM = Canadian Occupational Performance Measure; COPM-P = COPM-Performance; COPM-S = COPM-Satisfaction; PVQ = Pediatric Volitional Questionnaire; GAS = Goal Attainment Scaling.
Both interventions met the prespecified feasibility criteria, and no adverse events were reported (Table 4). Both SRP and HEP met the prespecified success threshold (≥75%) across adherence and fidelity indicators, and no adverse events were reported during the intervention period.
Table 4. Implementation Fidelity and Safety
| Indicator domain | Outcome metric | Planned dose / contacts | Success criterion | SRP (attendance-based) (n=8) | HEP (execution-based) (n=8) | Feasible |
|---|---|---|---|---|---|---|
| Adherence | Session completion rate (%) | SRP: 16 supervised sessions / HEP: 24 home sessions | ≥ 75% | 86.0 ± 7.3 | 89.1 ± 7.3 | Met |
| Structured feedback / contact fidelity | Engagement in structured feedback (%) | SRP: therapist feedback documentation / HEP: 8 planned coaching contacts | ≥ 75% | 89.2 ± 11.9 | 87.5 ± 9.4 | Met |
| Exercise exposure | Weekly exercise time (min/week) | Planned 90 min/week (8 weeks) | ≥ 67.5 min/week (≥75% of planned) | 77.4 ± 6.6 | 80.2 ± 6.6 | Met |
| Total exercise dose | Total exposure over 8 weeks (min) | Planned 720 min (90×8) | ≥ 540 min (≥75% of planned) | 619 ± 52 | 641 ± 53 | Met |
| Safety | Adverse events | Monitored during the intervention | None (target) | None reported | None reported | Met |
Note. Values are mean ± SD. Feasible indicates ≥75% of the prespecified criterion. No adverse events were reported. Structured feedback (%) reflects documented therapist feedback (SRP) and completed coaching contacts (HEP).
4. Discussion
This exploratory, low-risk QI pilot study compared an 8-week hospital-based SRP with a caregiver-led HEP in children with developmental disabilities classified as GMFCS I-III. Both models met the prespecified adherence threshold (≥75%) and no adverse events were reported, indicating the feasibility and safety of both delivery approaches. Activity-level outcomes (GMFM and PBS) improved over time in both groups, whereas participation-related outcomes (COPM and PVQ) showed differential change over time in a direction favoring SRP, suggesting that delivery context may influence perceived performance and session engagement beyond exercise prescription alone (Andersen et al., 2005; Franjoine et al., 2003; Law et al., 1990; Rosenbaum & Stewart, 2004; Russell et al., 1989). Given diagnostic heterogeneity and the conservative use of GMFCS as a functional descriptor, diagnosis-specific generalisation should be cautiously made. The significant time effects for GMFM and PBS suggest improvement in activity-related outcomes over time. This aligns with the ICF-based activity framework (Rosenbaum & Stewart, 2004) and the established responsiveness of the GMFM to repeated assessments (Russell et al., 1989). Furthermore, activity-related measures may improve with repeated task-oriented practice even in the absence of between-group differences. Both interventions involved task-oriented motor practice with comparable planned (90 min/week) and observed (approximately 77-80 min/week) exercise volumes. These shared features, together with aligned intensity targets (OMNI-RPE 5-7), may have contributed to the comparable activity outcomes, consistent with evidence highlighting the relevance of training volume and intensity for GMFM change (Hsu et al., 2019). Although total exercise time was similar, the two intervention models differed in delivery context and session frequency (2 supervised vs. 3 home sessions/week), which may have independently influenced engagement and participation. However, improvements in activity should not be assumed to translate directly into broader participation, which is influenced by environmental and contextual factors (Imms et al., 2017; Marinič, 2023; Rosenbaum & Stewart, 2004). For COPM and PVQ, significant group-by-time interactions suggest differential change between SRP and HEP over time, with the pattern favoring SRP (Andersen et al., 2005; Rosenbaum & Stewart, 2004). A plausible explanation is that SRP provided richer contextual supports, including immediate feedback (knowledge of results/knowledge of performance), structured scaffolding through graded task difficulty, and opportunities for peer interaction, which may have supported competence and relatedness, thereby influencing motivation and engagement (Ryan & Deci, 2000). Moreover, the supervised social context of the SRP may have provided opportunities for therapeutic alliance and peer interaction, both of which have been described in the pediatric rehabilitation literature as important facilitators of participation (Crom et al., 2020; Maciver et al., 2019). This pattern is broadly consistent with literature suggesting that contextual and interpersonal supports may shape participation experiences beyond activity-level change. This interpretation aligns with the view that participation is both a process and an outcome in childhood disability and that participation experiences may relate to broader social participation and family-perceived quality of life (Bulić et al., 2025; Imms et al., 2017). Simultaneously, several measurement considerations temper interpretation. The COPM ratings were based on standardised common goals rather than individualised goals, which may reduce the person-centered meaning of the COPM (Law et al., 1990). The PVQ is an observational measure anchored to the session context, and scores may be influenced by differences in delivery environments and baseline levels (Andersen et al., 2005). Accordingly, these findings should be viewed as preliminary evidence that contextual and interpersonal supports may amplify engagement and volition, rather than definitive evidence of SRP superiority (Ryan & Deci, 2000). The absence of between-group differences in GAS T-scores at T1 may reflect measurement design rather than true equivalence. The GAS was developed to capture individualised, meaningful change (Kiresuk & Sherman, 1968). In this study, standardised common goals were applied to improve comparability, which may have reduced responsiveness and content validity relative to individualised goal setting. In addition, GAS T-scores were derived at a single post-intervention time point, limiting the interpretation of individual trajectories and change patterns. Thus, the GAS findings may indicate that common-goal GAS designs are less sensitive to small, individualised changes than traditional individualised GAS approaches, in which goals and attainment levels are tailored to the participant's baseline and functional contexts (Steenbeek et al., 2007). This study addressed potential reporting bias in home-based interventions by reporting multidimensional fidelity indicators (session attendance/completion, coaching participation, weekly exercise time, and total dose) rather than relying on a single adherence metric (Bollen et al., 2014). Standardised caregiver training and structured weekly coaching may also enhance the reproducibility of HEP delivery and align with evidence that caregiver barriers and psychosocial determinants influence adherence in pediatric disability (Lillo-Navarro et al., 2019; Niyonsenga et al., 2024; Novak & Končar, 2022). Although the present findings do not directly support a specific delivery strategy, the differing contextual characteristics of SRP and HEP may inform future research on combined or sequential models. SRP may support skill acquisition and engagement through structured feedback and peer interaction, whereas HEP may facilitate repetition and generalisation in daily contexts (Rosenbaum & Stewart, 2004; Ryan & Deci, 2000). When HEP-only delivery is necessary, explicit caregiver training specification, coaching frequency, feedback modalities, and barrier management may be critical for optimising implementation and outcomes (Lillo-Navarro et al., 2019; Niyonsenga et al., 2024). Future work should explicitly define and report coaching, practice conditions, and feedback strategies across settings to clarify active ingredients (Levac et al., 2009).
4.1. Limitations
Several limitations should be noted. As this is a single-center exploratory study with a small sample (n = 16), the results are not generalisable, and session frequency could not be included as a covariate in the statistical model. Additional constraints include diagnostic heterogeneity, conservative use of the GMFCS, PVQ context dependence, reduced responsiveness due to the common-goal GAS approach, and the absence of long-term follow-up (Andersen et al., 2005; Steenbeek et al., 2007).
4.2. Future Directions
Future studies should recruit larger samples with functional level stratification and incorporate 3-6-month follow-up assessments. Measurement rigor should be strengthened using PVQ scoring based on recorded sessions to improve standardization. A mixed GAS approach that combines individualised goals with standardised scoring rules may better balance clinical meaning and comparability. Finally, family-level outcomes should be included, and models to identify which families benefit the most from HEP may improve targeting.
5. Conclusion
Both SRP and HEP were feasible and safe, meeting the prespecified adherence thresholds without adverse events. Activity-level outcomes improved over time in both groups, while SRP showed more favorable patterns in participation-related outcomes and therapy engagement. Future studies may explore how the differing contextual strengths of SRP and HEP can inform alternative delivery models. The authors declare no conflicts of interest.
References
- Andersen, S and Kielhofner, G and Lai, J.-S (2005). An examination of the measurement properties of the Pediatric Volitional Questionnaire.
- Ballantyne, M and Liscumb, L and Brandon, E and Jaffar, J and Macdonald, A and Beaune, L (2019). Mothers' perceived barriers to and recommendations for health care appointment keeping for children who have cerebral palsy.
- Bhat, A. N (2021). Motor impairment increases in children with autism spectrum disorder as a function of social communication, cognitive and functional impairment, repetitive behavior severity, and comorbid diagnoses: A SPARK study report.
- Bishop, J. C and Pangelinan, M (2018). Motor skills intervention research of children with disabilities.
- Bollen, J. C and Dean, S. G and Siegert, R. J and Howe, T. E and Goodwin, V. A (2014). A systematic review of measures of self-reported adherence to unsupervised home-based rehabilitation exercise programmes, and their psychometric properties.
- Bulić, D and Ljutic, T and Pinjatela, R (2025). Family Quality of Life from the Perspective of Parents of Children with Intellectual Disabilities. Journal of health and rehabilitation sciences, 4.
- Crom, A and Paap, D and Wijma, A and Dijkstra, P. U and Pool, G (2020). Between the lines: a qualitative phenomenological analysis of the therapeutic alliance in pediatric physical therapy.
- Franjoine, M. R and Gunther, J. S and Taylor, M. J (2003). Pediatric balance scale: a modified version of the berg balance scale for the school-age child with mild to moderate motor impairment.
- Guralnick, M. J (2011). Why early intervention works: A systems perspective.
- Healy, S and Nacario, A and Braithwaite, R. E and Hopper, C (2018). The effect of physical activity interventions on youth with autism spectrum disorder: A meta‐analysis.
- Hsu, C.-W and Kang, Y.-N and Tseng, S.-H (2019). Effects of therapeutic exercise intensity on cerebral palsy outcomes: a systematic review with meta-regression of randomized clinical trials.
- Imms, C and Granlund, M and Wilson, P. H and Steenbergen, B and Rosenbaum, P. L and Gordon, A. M (2017). Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability.
- King, S and Teplicky, R and King, G and Rosenbaum, P (2004). Family-centered service for children with cerebral palsy and their families: a review of the literature.
- Kiresuk, T. J and Sherman, R. E (1968). Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community mental health journal, 4.
- Law, M and Baptiste, S and McColl, M and Opzoomer, A and Polatajko, H and Pollock, N (1990). The Canadian occupational performance measure: an outcome measure for occupational therapy. Canadian journal of occupational therapy, 57.
- Leon, A. C and Davis, L. L and Kraemer, H. C (2011). The role and interpretation of pilot studies in clinical research. Journal of psychiatric research, 45.
- Levac, D and Wishart, L and Missiuna, C and Wright, V (2009). The application of motor learning strategies within functionally based interventions for children with neuromotor conditions.
- Maciver, D and Rutherford, M and Arakelyan, S and Kramer, J. M and Richmond, J and Todorova, L and Romero-Ayuso, D and Nakamura-Thomas, H and Ten Velden, M and Finlayson, I (2019). Participation of children with disabilities in school: A realist systematic review of psychosocial and environmental factors.
- Marinič, I (2023). Review of Educators' Needs for Additional Knowledge About Autism in Slovenia. Journal of Health and Rehabilitation Sciences, 2.
- Medicine, A. C. o. S (2009). American College of Sports Medicine position stand.
- Niyonsenga, J and Uwingeneye, L and Musabyemariya, I and Sagahutu, J. B and Cavallini, F and Caricati, L and Eugene, R and Mutabaruka, J and Jansen, S and Monacelli, N (2024). The psychosocial determinants of adherence to home-based rehabilitation strategies in parents of children with cerebral palsy: A systematic review.
- Novak, I and Mcintyre, S and Morgan, C and Campbell, L and Dark, L and Morton, N and Stumbles, E and Wilson, S. A and Goldsmith, S (2013). A systematic review of interventions for children with cerebral palsy: state of the evidence.
- Novak, M and Končar, M (2022). Role of gender and age in the cooperation between parents of people with intellectual disabilities and professional staff in care centres. Journal of Health and Rehabilitation Sciences, 1.
- Palisano, R and Rosenbaum, P and Walter, S and Russell, D and Wood, E and Galuppi, B (1997). Development and reliability of a system to classify gross motor function in children with cerebral palsy.
- Rosenbaum, P and Stewart, D (2004). The World Health Organization International Classification of Functioning, Disability, and Health: a model to guide clinical thinking, practice and research in the field of cerebral palsy.
- Ruggeri, A and Dancel, A and Johnson, R and Sargent, B (2020). The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: A systematic review.
- Russell, D. J and Rosenbaum, P. L and Cadman, D. T and Gowland, C and Hardy, S and Jarvis, S (1989). The gross motor function measure: a means to evaluate the effects of physical therapy.
- Ryan, R. M and Deci, E. L (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being.
- Steenbeek, D and Ketelaar, M and Galama, K and Gorter, J. W (2007). Goal attainment scaling in paediatric rehabilitation: a critical review of the literature.
- Tatla, S. K and Sauve, K and Virji‐Babul, N and Holsti, L and Butler, C and Van Der Loos, H. F. M (2013). Evidence for outcomes of motivational rehabilitation interventions for children and adolescents with cerebral palsy: an American Academy for Cerebral Palsy and Developmental Medicine systematic review.
- Thabane, L and Ma, J and Chu, R and Cheng, J and Ismaila, A and Rios, L. P and Robson, R and Thabane, M and Giangregorio, L and Goldsmith, C. H (2010). A tutorial on pilot studies: the what, why and how.
- Utter, A. C and Robertson, R. J and Nieman, D. C and Kang, J (2002). Children's OMNI scale of perceived exertion: walking/running evaluation.
- Xie, Y and Wu, J and Li, Y and Liu, H and Peng, Y and Zhou, P and Sun, Y and Kang, L and Jiang, C and Wu, H (2024). Requirements for and barriers to rehabilitation services for children with disabilities in middle-and high-income countries: Scoping review. Interactive journal of medical research, 13.